medical history - Hagerstown Dermatology & Skincare
advertisement

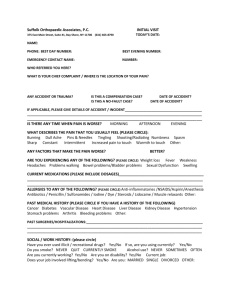
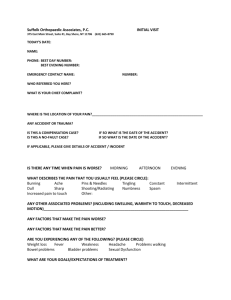
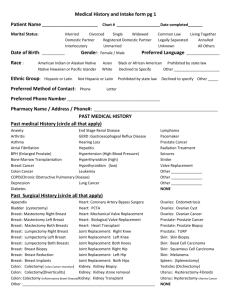
MEDICAL HISTORY Patient name: ___________________________________________________________________ Reason for today’s visit? ___________________________________________________________ - How long has this been a problem? _________________________________ - Have you tried any treatments or medications in the past for your current condition? YES NO If yes, please list medications and over the counter items you have tried: ___________________________________________________________________________ Pharmacy Name/Address: _________________________________________________________ Current Medications If N/A - Circle NONE Include prescriptions, over-the-counter meds (such as aspirin), vitamins, supplements and herbal products: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Allergies If N/A- Circle NONE List all medications, seasonal/environmental, foods, adhesive, latex – and include reactions: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Female patients: Pregnant? ______ Planning a pregnancy? ______ Currently Breastfeeding? ______ Birth control? If yes, please list name of pill, or contraception method you are using currently: _____________________________________________ Past Medical History: (Please circle all that apply) Arthritis/Joint problems GERD/Esophageal Reflux Pacemaker Anxiety Hearing Loss Radiation Treatment Asthma HIV infection/ AIDS Seizures Atrial Fibrillation (Irregular Heartbeat) Hepatitis Stroke Blood clots or clotting disorder Hypercholesterolemia Varicose Veins Bronchitis Hypertension/blood pressure problems Cancer (what type) ___________________ Hyperthyroidism COPD Hypothyroidism Coronary Artery Disease Leukemia Depression Lymphoma Diabetes Lupus Fainting Night Sweats Other:________________________________________________________________________________ Past Surgical History: (Please circle all that apply) Appendix Removed Bladder Breast: Mastectomy R L Both Breast: Lumpectomy R L Both Breast Biopsy Breast Reduction Breast Implants Colectomy: Colon Cancer Resection Colectomy: Diverticulitis Colectomy: Inflamm. Bowel Disease Gallbladder Heart: Coronary Artery Bypass Heart: Mechanical Valve Replacement Skin Biopsy Heart: Biological Valve Replacement Skin Cancer: Joint Replacement: Knee R L Both Basal Cell Joint Replacement: Hip R L Both Squamous Cell Kidney Biopsy Melanoma Kidney Removed R L Both Spleen Removal Kidney Stone Removal Hysterectomy: Ovaries Removed: Cyst Fibroids Tubal Ligation Uterine Cancer Endometriosis Testicle Removal Ovarian Cancer Tonsillectomy Prostate Removed: Cancer Other: _____________________ Personal Skin History: (Please circle all that apply) Acne Actinic Keratosis (Pre-cancers) Asthma Basal Cell Skin Cancer Dry Skin Eczema Flaking or Itchy Scalp Hay Fever/Allergies Melanoma Poison Ivy/Rashes Atypical/“Pre-Cancerous” Moles Squamous Cell Skin Cancer Psoriasis Warts Cold Sores Blistering Sunburns Significant sunburns Infection/MRSA Tanning bed use? Current _____ Past ______ For how long/how often? ____________________________________________________ Sunscreen use (circle): Daily Occasionally Only at the Beach I don’t use sunscreen Social History: Smoking: Current every day smoker _____ Current some day smoker (tobacco)____ Current some day smoker (cigarette)____ Alcohol: None ______ 1-2 drinks/day_____ Never Smoker_____ Former Smoker_____ less than 1 drink/day_____ 3 or more drinks/day_____ Family History (blood relative i.e., grandmother, brother, child.) Acne _______________________ Allergies/Hayfever _____________________________ Eczema _____________________ Psoriasis _____________________________________ Auto-Immune Disorders (thyroid, Lupus, M.S., Vitiligo) ______________________________ Other: _____________________________________________________________________ Skin Cancer _______________________________ Type? (Circle) Basal Cell Carcinoma Squamous Cell Carcinoma Melanoma Please check here if you are interested in receiving more information about: Chemical Peels _____ Skin Care/Anti-Aging Products _____ Sun Protection/Sunscreens _____ Treatment of Excessive Underarm Sweating _____ Wrinkle relaxers (Botox, Dysport) _____ Spider Veins on the legs (Sclerotherapy) _____ Wrinkle fillers (Restylane, Juvaderm) _____ REQUEST FOR CONFIDENTIAL COMMUNICATIONS I request that all communications to me (via telephone, mail or otherwise) by Hagerstown Dermatology and Skin Care and/or its staff are handled in the following manner: For written communications: (Mailing address) ________________________________________________________________ For oral communications: (Telephone number) _______________________________________________________________________________ Email Address: ________________________________________________________________ Would you like to receive information on specials, or relevant information? Yes No Do we have permission to: Leave a message on your machine at home? YES Leave a message at your place of employment? NO YES NO Discuss your Medical Condition or results with any member of your household? YES NO If Yes, Whom: _______________________________________________________________ Relationship:_________________________________________________________________ _________________________________________ ____________________ Patient Signature Date