Myoblast transplantation for Duchenne Muscular Dystrophy By
advertisement

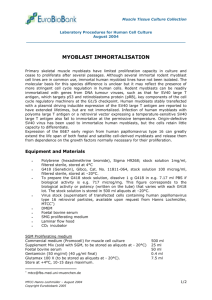
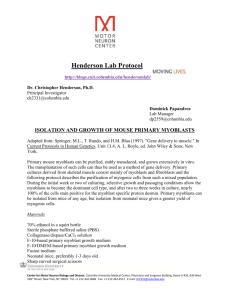
Myoblast transplantation for Duchenne Muscular Dystrophy By Jacques P. Tremblay Muscle fibers are the only cells in the human body that contain more than one nucleus. It is because they are formed during embryogenesis by the fusion of thousands of mono-nucleated cells called myoblasts. A special stem cell, called the satellite cell, is also located near the muscle fibers. This satellite cell is normally quiescent. However, when the muscle fibers are damaged the satellite cells receive signal to proliferate and differentiate into myoblasts, which fuse with the damaged muscle fibers to repair it. This fusion of the myoblasts with the muscle fibers thus introduces new nuclei inside the muscle fibers. Myoblasts can be proliferated in culture from the satellite cells present in a muscle biopsy. Several million myoblasts can be obtained from a single satellite cell. Duchenne Muscular Dystrophy (DMD) is due to the absence of dystrophin in the muscle fibers of the patients. In 1989, Dr. Partridge was the first to transplant myoblasts obtained from a healthy mouse in the muscles of mouse model (called the mdx mouse) of DMD. As the DMD patients, the mdx mice have no dystrophin in their muscle fibers. The myoblasts of the healthy mouse fused with the damaged muscle fibers of the mdx mice and thus introduced in these fibers the donor nuclei, which contain the normal dystrophin gene. This led to the expression of dystrophin in the muscle fibers containing the nuclei of the healthy myoblasts. This result of Dr. Partridge led to several clinical trial of myoblast transplantation on the muscles of Duchenne Muscular Dystrophy patients. These clinical trials were conducted by several research groups conducted by Drs. Karpati, Law, Gussoni, Miller, Mendell and myself. These early clinical trials produced rather poor results because the parameters of this type of cellular transplantation had not been sufficiently investigated in animal models before these early clinical trials. The problems that were not sufficiently investigated were the number of myoblasts to be transplanted per muscle, the distance between the injection trajectories, the type of immunosuppressive treatment necessary to prevent the rejection of the donor myoblasts. In the scheme above, a muscle biopsy is done on a healthy donor. The satellite cells present in this muscle biopsy are isolated and expanded as myoblasts 20 million folds in culture. These normal myoblasts are then injected in the muscle of a Duchenne patient. These myoblasts fused with the muscle fibers of the patients and thus introduce in these muscle fibers their nuclei containing the normal dystrophin gene. This led to the expression of dystrophin by these fibers. Since these early clinical trials my research groups has done many myoblast transplantation experiments not only in mdx mice but also in monkeys, which is a larger animal model more similar to humans. We have transplanted myoblasts obtained from a biopsy of his father in the muscles of a 26 years old DMD patient. After 18 months of immunosuppression with tacrolimus to prevent the immune rejection of the father cells, we observed the expression of dystrophin in up to 34% of the fibers in a muscle transplanted with the myoblasts. We have also conducted a new phase I clinical trial on 9 DMD patients that ended in 2005. In that clinical trial the patients were transplanted with myoblasts obtained from their father or their mother. The myoblasts were transplanted in only one centimeter cube of muscle. The patients were immunosuppressed with tacrolimus. The muscle site injected with myoblasts was biopsied 1 month later. In each of the 9 patients we detected the presence of the normal dystrophin gene and the presence of dystrophin positive fibers in up to 26% of the fibers. The results of that clinical trial were thus rather encouraging. The figure above illustrates the expression of dystrophin in 26% of the muscle fibers in a Duchenne Muscular Dystrophy patient one month after the transplantation of myoblasts obtained from a healthy donor. Since 2005, we have been delayed form doing a Phase II clinical trial of myoblast transplantation to DMD patients. One of the main constrain is that the ethic committee of my hospital requested that the DMD patients should be more than 18 years old. The regulatory authority for clinical trial in Canada (Health Canada) also requested that the patients should not be on a respirator, should not be positive for the cytomegalovirus and should be within 1 hour of driving from the research center. Since the clinical trial aimed to verify whether the transplantation of myoblasts throughout a forearm muscle could increase the strength of that muscle, the clinical trial also required that the patients be able to move both wrists. Since that time no patient was able to fulfill all the requirements. We now have the permission of an ethic committee for a hospital in London (Ontario, Canada) to include patients, who are above 16 years old. We have also obtained grants from the Foundation for Cell and Gene Therapies and from the Canadian Institute of Health Research to conduct this new trial. We hope to be able to start this new trial in March 2014. This trial will include only patients that will be located within one hour of driving from London. However, the major limitation of myoblast transplantation is that these cells have to be transplanted in each muscle since they do not migrate from the injection sites because they are attracted only by the damaged muscle fibers. To overcome this limitation, other research groups are also working on the transplantation of other types of cells, which could be injected in the blood of the patients and migrate in the muscles. Dr. Torrente is working on the transplantation of CD133 cells and Dr. Cossu has initiated a clinical trial of mesoangioblast transplantation. The readers are invited to read the summaries provided by these investigators on the web site of the International Consortium of Gene Therapy. Cell therapies for DMD have the advantage that this is the only type of treatment, which could eventually increase the capacity of the muscles of the DMD patients to repair themselves.