P225 Renal disease in patients treated with alemtuzumab for
advertisement

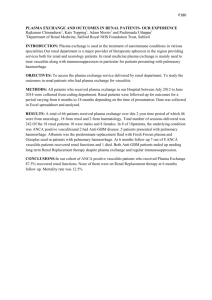
P225 Renal disease in patients treated with alemtuzumab for multiple sclerosis Phelps, RG Renal Autoimmunity Group, Queen’s Medical Research Institute, University of Edinburgh INTRODUCTION: De novo autoimmunity occurs in more than a third of patients treated with alemtuzumab (AZ) for multiple sclerosis (MS). Autoimmune thyroid disease and thrombocytopenia are most common, but renal autoimmune conditions including Goodpasture’s disease (GD) and membranous nephropathy (MN) have been reported, some patients developing endstage renal failure (ESRF). AZ is increasingly recognised as one the most effective treatments for MS. With its new licensing in Europe (2013), it is timely to review the occurrence of renal autoimmunity in AZ-treated patients with MS. METHODS: Cases were identified by a search of MEDLINE and through correspondence with Genzyme, the company developing AZ for use in MS, which shared records of all cases reported to them in the course of the pre-marketing trials program. RESULTS: Seven patients (all female) are known to have developed autoimmune renal diseases after AZ treatment of their MS (Figure 1), all within 4 years of 1-3 courses of AZ. Although only 0.3% of AZ-treated MS patients have developed renal autoimmunity, the incidence is vastly greater than in the general population (~700x for GD and ~10x for MN). Three patients developed ESRF due to Goodpasture’s disease: onset in 2 (B and G) was subacute such that early recognition and appropriate treatment might have been effective, as it was in a 4th case of GD which occurred within a clinical trial. Two patients developed MN presenting with nephrotic syndrome and so far stable renal function. One patient (case D) with renal function and biopsy findings consistent with MN as the sole diagnosis was treated as GD because of a rising titre of anti-GBM antibodies in serum. Figure 1: Goodpasture's disease and membranous nephropathy in AZ-treated patients with MS. CONCLUSION: There is increased risk of autoimmune renal disease in the 4 years after AZ treatment for MS. At least some cases of GD have had sub-acute presentations such that close surveillance could enable early successful treatment. It is not yet clear if sub-acute presentations of GD are peculiar to this clinical setting or are affording new insight to the natural history of a disease that generally presents as a fulminant illness with little or no prodrome.