Infrastructure Unit Systes Support (IUSS) Project
advertisement
 Project")
IUSS HEALTH FACILITY
GUIDES
Paediatrics & Neonatology
Units
[DISCUSSION DRAFT 1]
10 June2012
supportedby:
INFORMATION
Form
Status
Notes
Health facility guides.
Discussion document, draft 1, current, not binding, 20 May 2012
TITLE
Neonatal Unit
Description
Reference
Authors
Active
stakeholder’s list
Endorsements
Endorsements
pending
Supersedes
Action
required
Y/N
Correspondence
“Neonatal unit” contains health facility guidance in five parts covering
the infrastructure norms and standards for neonatal unitsfor facilities
providing regional, tertiary, central and national referralservices. It is to
be read in conjunction with the full norms and standards suite and
covers policy and service context (Part A)planning and design (Part B),
room data (Part C), accommodation schedules, (Part D) and case
studies (Part E)
CSIR ...............................
IUSS NandStask team020
Departments of health or departments of health and social
development in the Eastern Cape, Free State, KwaZulu-Natal, Limpopo,
Mpumalanga, Northern Cape, North West, and Western Cape
provinces
Department of public works or department of transport and public
works in the Eastern Cape, KwaZulu-Natal, and Western Cape
The National Department of Health
The document is endorsed by the CSIR
Submitted to the IUSS Norms and Standards Working Group for
endorsement
N/A
Description:
By whom:
By when:
IUSS@csir.co.za Building Science and Technology, CSIR Built
Environment
Box
395,
PRETORIA,
0001,
South
Africa.
Peta
de
Jagerpdejager@csir.co.za
Accessing of these guides
This publication is received by the National Department of Health (NDoH), IUSS Steering Committee Chairman:
Dr Massoud Shaker.
Use of text, figures or illustrations from this report in any future documentation, media reports, publications,
competition entries and advertising or marketing material is solely at the discretion of the IUSS Steering
Committee and Working Group and should clearly reference the source. This publication may not be altered
without the express permission of the IUSS Steering Committee and Working Group. Feedback is welcome.
This document (or its updates) is available freely at www.iussonline.co.za
Disclaimer
This is a discussion draft guidance document has been prepared in the development of national Norms and
Standards for the National Department of Health for the benefit of all South Africans involved in the
procurement, design, management and commissioning of healthcare infrastructure across both public and
private sectors. Use of the guidance in this document is at the risk of the implementing party, until endorsed
by the National Health Council of the Department of Health.
Development status
The development process adopted by the IUSS team is to consolidate information from a range of sources
including local and international literature, expert opinion, practice and expert group workshop/s into a first
level discussion status document. This will then be released for comment through the iussonline website and
through IUSS, national and provincial channels. Feedback and further development will be consolidated into a
second level development status document which again will be released for comment and more rigorous
technical review. Further feedback will be incorporated into proposal status documents for formal submission
to the Department of Health Technical Review Committee. Once approved documents will be submitted for
formal approval by the National Health Council at which stage documents reach approved status. At all
development stages documents may go through various drafts and the final approved document will be
assigned a version number. Documents may be used at risk for project development at all development stages
but will only become mandatory in final approved status.
Acknowledgements
This publication has been funded by the NDoH.
IUSS NandS task team 020(ntensive care units): Edwina Fleming, Etha van der Schyf, Geoff Abbott, Magda
Coetzer and Nkhensani Baloyi
Table of Contents
PART A – POLICY AND SERVICE CONTEXT………………………………………………………………………………………….…………1
Overview………………………………………………………………………………………………………………………………………….1
Policy Context………………………………………………………………………………………………………………………………….1
PART B – PLANNING AND DESIGN………………………………………………………………………………………….……………………4
Overview…………………………………………………………………………………………………………………………………………4
Scope………………………………………………………………………………………………………………………………………………5
Departmental Functional Relationships……………………………………………………………………………….………....9
Patient Flow………………………………………………………………………………………………………………………….…………9
Flow Diagram……………………………………………………………………………………………………………………….…………9
Area 1 –Entrance and waiting…………………………………………………………………………….…………………………13
Area 2 –Assessment………………………………………………………………………………………..……………...……………..13
Area 3 –Treatment…………………………………………………………………………………………...….……….……………….14
Resuscitation area (Code Red)…………………………………………………………………………………………….…………14
Acute treatment area (Codes orange and yellow)…………………………………………………………….…..………18
Consultation area (Code green)…………………………………………………………………………………….………………20
Shared facilities…………………………………………………………………………………………………………….….……….…..21
Special areas – Mental Health assessment………………………………………………………………….….……………..21
Special areas – Crisis Centre…………………………………………………………………………….………….……….………..23
PART C – ACCOMODATION SCHEDULES…………………………………………………………………………………………………….24
PART D –ROOM DATA…………………………………………………………………………………………………………………….…….……26
LIST OF ABBREVIATIONS…………………………………………………………………………………………………………………………….28
PART A – Policy and service context
Overview
A Neonatal Care Unit is a discrete and
environmentally controlled unit designed,
equipped and staffed to care for premature
and medically unstable or critically ill
newborns who require more than the
routine care provided in maternity
The neonatal unit provides care for neonates who require more than the
routine care provided in maternity units. This includes cot space provision
for standard care, high dependency care and intensive care, and the
associated clinical and non-clinical support facilities, including facilities for
families .
This document provides guidance on the neonatal unit that admit patients
whose dependency levels are classified as level 2 or 3 as defined (xxxrefThis
document describes spaces that are unique to neonatal units and is to be
read in conjunction with the full IUSS suite see IUSS documents map. It also
describes common variations to hospital spaces and clarifies requirements
for these spaces, where necessary.It recommends minimum space, functional
layouts, patient handling, infection prevention, architectural detail, and surface and furnishing needs for clinical and
support areas. The document also addresses minimum engineering design criteria for plumbing, electrical, and heating,
ventilation, and air-conditioning (HVAC) systems.
Examples of space requirements for a typical neonatal unit are contained in PART C schedules of
accommodation The example schedules provide a basis for sizing facilities at initial planning stages but exact
requirements should be determined locally based on the number and case mix of patients, hospital policy for
the provision of supplies and waste disposal, and the layout of the unit.
Policy context
Service context:
According to Government Notice - R. 655 National Health Act 61/2003:
Regulations: Categories of hospitals : No.34521
The hospital will provide emergency care in accordance with the service package for District services and will
refer more complex patients to the level 2 hospitals at xx hospital. Level 3 patients will be referred to the xx
tertiary hospital
a)
District hospital A district hospital may provide standradard care of neonates
c)
Regional hospital – “
A regional hospital may provide neonatal care for standradard care, high dependency care and
intensive care of neonates,
d) Tertiary hospitals –
A tertiary hospital may provide a specialist neonatal services,
e)
Central hospitals Central referral services are provided in highly specialised units, require unique, highly skilled and
scarce personnel and at a small number of sites nationwide
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
1
Service Context
Bed Allocation for newborns and children
Total hospital beds
District hospital
Regional hospital
Tertiary hospital
0,7 - 1,3 / 1 000 local population
0,3 - 0,5 / 1 000 regional population
0,2 - 0,3 / 1 000 tertiary population
Hospitals with 2 levels of care need to calculate the bed allocation for each level on the basis of the
catchment population for that level.
Children's beds
District hospital
Regional & tertiary
Neonatal beds**
District hospital
Regionalhospital
Tertiary hospital
20% of hospital beds to be allocated to neonates & children
20% of hospital beds to be allocated to neonates & medical
children
3-4 / 1 000 local deliveries
1,5 / 1 000 deliveries in level 2 catchment area
0,5 / 1 000 deliveries in level 3 catchment area
Hospitals with 2 levels of care need to calculate the bed allocation for each level on the basis of the
number of deliveries in the catchment area of each level.
Paediatric beds
Total children's beds less neonatal beds.
Norms extracted from KZN DoH 1999 STP &NDoH 2006 STP
** Norms adapted from Adhikari, Cooper, Jones& Woods. Summary of Health Plan for Neonatal
Care, 1997
Function of beds:
Allocation of beds is according to function & should be in the proportions in the table below.
Neonatal
Paediatric
Standard
High care
ICU
KMC
Total
General
Isolation
High care*
ICU#
Total
District
Regional
Tertiary
34%
33%
34%
23%
10%
33%
100%
64%
25%
8%
3%
100%
15%
50%
30%
5%
100%
72%
15%
8%
5%
100%
33%
100%
59%
33%
8%
100%
* Add an additional 2 beds to Level 2 and Level 3 hospitals for surgical children
# Add an additional bed to 2 beds to Level 2 hospitals for surgical children
Never mix children on adult wards
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
2
Provision for Children in the Hospital
Level of
Population Beds per
Service
served
1000
population
Level 1/
300,000
0.7-1.3
District
beds
Doctors
Placement
Outpatients
Generalist
Nursery is
component
of
maternity
unit
Dedicated
childrens
component
in OPD
Teaching
Childrens’
Wards
20% beds
allocated
for children
split into
newborn
and
children
Children –
medical
and
surgical,
dedicated
ward for
both
Separate
wards
medical
and
surgical
Dedicated
paediatrics
Level 2
/Regional
1,2million
0.3-0.5
beds
Specialists
dedicated
Stand alone
nursery
adjacent to
maternity
Dedicated
childrens
OPD
Teaching
function
20% beds
for medical
children
Level 3/
Tertairy
3,5million
0.2-0.3
beds
Specialists
and sub
specialists
Stand alone
nursery
Dedicated
childrens
OPD
Teaching
function
20% beds
for medical
children
It is recommended that considerable flexibility is maintained within a neonatal unit. A baby’s care
requirements may change between intensive care and high dependency care and it is preferable not to move
the baby. High dependency areas should therefore be equipped to enable intensive care to take place.
Some designated h care and high dependency care rooms should also be equipped for intensive care, as this
allows emergency movement of infants from intensive care in the event of fire. It also allows high care cots to
be used for intensive care at a time when an outbreak of infection has occurred in the intensive care rooms
('Designing a neonatal unit'; BAPM, 2004).
Standard (intermediate)
High Care
ICU
KMC (low care)
District
34%
34%
Regional
34%
23%
10%
33%
33%
Tertiary
15%
50%
30%
5%
Minimum size of a neonatal unit is 6 beds
Hours of operation:
The Neonatal Unitoperates 24 hours per day, seven days per week24 hours
Parents will have round-the-clock access to the Unit.
Emergency admissions will be from the Delivery Suite, Operating Suite or external retrieval so 24 hour
readiness for admissions is essential.
Staff:
Staff who will be present in the Neonatal Unit include unit-based nursing staff that provide continuous care to
patients in shifts, visiting clinical staff who call to provide periodic or specialised care to patients (such as
medical doctors and allied healthcare workers and persons who provide support services (such as cleaning
staff and maintenance staff). Visiting and teaching activities may also take place.
Staff numbers are dependent on the activities provided within the NU
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
3
PART B – Planning and design
Overview
The service and policy
context should be the
basic determinant
ofplanning and design
principles in the
Neonatal Unit design.
The national and provincial service and policy context (Part A) is the basic
determinant of planning and design principles.Part B contains planning and design
guidance, design considerations, functional relationships between hospital
departments with respect to emergency centre (EC), and relationships within the
EC. These principles are subsequently developed into a series of schedules of
accommodation. (Part C), room data sheets (Part D) including some indicative
equipment lists and case studies (Part E). Parts C, D and E are intended to
demonstrate how the principles prescribed in Part B can be applied in worked
examples. Parts C or D if used directly are deemed-to-satisfy the principles
developed in Part B, but are not the only acceptable solutions.
Case studies (Part E) are for illustrative purposes to demonstrate worked solutions
and should not be adopted without appropriate contextual adaptation.
Levels of neonatal care
There are three categories of care above and beyond the routine care provided in a maternity unit:
Standard Care
The Standard Care Nursery caters for newborns requiring less care and supervision -although not
necessarily excluding respiratory support - but who are not sufficiently stable to be discharged, and it
may serve as a stepdown from intensive care.It includes the care of less immature premature babies
who no longer need high dependency or intensive care while they grow to a stage of maturity ready for
discharge. This includes tube feeding, maintenance of body temperature and monitoring; and the care
of babies recovering from illnesses or operations, for example treatment of infections, jaundice and
special nutrition.
These may be babies with a birth weight of more than 1000 g and gestational age of more than 28
weeks. Continuous life support can be provided but is limited to conventional mechanical ventilation.
There will normally be a 1:4 ratio of staff to babies
High dependency care
High dependency care provides higher levels of clinical care including for neonates recovering from
intensive care. This includes babies receiving oxygen for immature lungs as they breathe on their own,
sometimes assisted by higher pressure given via nasal prongs; and babies on intravenous nutrition or
treated with chest drains or for convulsions, infections or metabolic problems.
These are babies with extremely low birth weight (1000 g or less) and 28 or less weeks' gestation
requiring advanced respiratory support such as high frequency ventilation and inhaled nitric oxide.
They require on-site access to a full range of paediatric medical subspecialties and medical imaging on
an urgent basis including CT, MRI and echocardiography.
There will normally be a 1:2 ratio of staff to babies.
Intensive care (NICU)
These are babies born prematurely, simply to support organ systems until they have matured; and
babies who are ill or who have life-threatening congenital disorders. Applies to babies requiring
continuous life support and comprehensive care for complex and critical illness and prematurity.
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
4
The greater the immaturity, the more needs to be done to support a baby’s breathing (often with
mechanical ventilation), and to protect it from infection and to achieve growth equivalent to that which
occurs in the womb. Thus, even babies who are otherwise well but very premature require intensive
care simply to support their life until their organ systems undergo maturity. This includes sophisticated
mechanical ventilation with oxygen, intravenous feeding, and the use of incubators to control body
temperature and protect from infection. It also involves treatment of illnesses that are more common in
such vulnerable babies.
Neonatal intensive care is also required for a small number of larger, more mature babies who become
ill from complications of delivery, from infection or metabolic disorders or when surgical or other
treatment is required for congenital anomalies such as congenital heart disease, disorders of the lung or
gut, or of other organs.
Intensive care, frequently needed for a period of weeks, is then followed by further weeks of high
dependency or special care provided in neonatal units as the babies grow to maturity
There will normally be a 1:1 ratio of staff to babies.
It is recommended that considerable flexibility is maintained within a neonatal unit. A baby’s care
requirements may change between intensive care and high dependency care and it is preferable not to move
the baby. High dependency areas should therefore be equipped to enable intensive care to take place.
Some designated h care and high dependency care rooms should also be equipped for intensive care, as this
allows emergency movement of infants from intensive care in the event of fire. It also allows high care cots to
be used for intensive care at a time when an outbreak of infection has occurred in the intensive care rooms
('Designing a neonatal unit'; BAPM, 2004).
Scope
The neonatal component of the maternity ward must:
be distinct from the maternal components
have no through traffic
have strict access control
comprise four major elements:
o rooming-in in all post natal cubicles
o a “well baby” facility
o Kangaroo Mother Care (KMC) unit
o a neonatal nursery for “small or sick babies”.
Rooming-in must be considered the norm.
Facilities must therefore provide adequate space to allow all babies to stay with their mothers.
Design and layout must be “baby-centred”, “family-centred” and must provide appropriate facilities for staff
comfort
BABY-CENTRED
Unit design must create an environment that:
- provides facilities to enable best clinical practice from full life support to convalescent care
- allows optimal infant development via attention to noise reduction, light and temperature controls
- allows easy family access 24 hours/day
- minimises risk of adverse occurrences, especially infection
- provides flexibility for future changes in practice and technology.
FAMILY-CENTERED
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
5
Unit design must recognize the pivotal role of the parents and other family members as part of the baby’s care
team. The environment must:
- create a welcoming entry
- provide adequate space and facilities for families at the cot side
- provide live-in parent accommodation within the Unit
- allow for privacy and encourage physical contact, attachment and breastfeeding / expression of breast milk
- provide quiet facilities for counselling, grieving and care planning
- provide “retreat” facilities
- facilitate communication with staff.
STAFF-ORIENTATED
Unit design must provide optimal working conditions and facilities for staff that provides / allows for:
- a pleasant and supportive working environment
- flexibility in staff allocation and ease of staff movement
- good access to and observation of patients. Observation may be direct and via remote monitoring
- implementation of good infection control and occupational health & safety practices
- appropriate information technology and communication systems
- staff lounge and adequate staff amenities
- continuing education and training facilities
- facilities for clinical research
- necessary office and administration space
Functional Areas
Space determinants revolve around the major functional areas:
PUBLIC SPACES
Entrances to the Unit
o
Reception, visitors waiting, ablutions
o
Family areas including a counselling room
o
Counselling room
o
Consulting room
CLINICAL SPACES
Rooming -in at all post natal cubicles,
A well baby facility,
Kangaroo Mother care (KMC) unit,
A neonatal nursery for sick or small babies providing,
o Standard care area
o High dependency care area
o Intensive care area
STAFF SPACES
Administrative area,
Staff Amenities, staff rest room and change room,
Overnight accommodation
SUPPORT SPACES
Clean utility,
Dirty utility,
Sluice
Stores
o
Surgical supplies
o
Clean linen,
o
Consumables,
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
6
o
Equipment,
o
Medical
Waste disposal,
Cleaners room,
Circulation space.
Ward kitchen
Ward laboratory
Clinical technologist office
Location
Relationships with the maternity unit
The neonatal unity should be adjacent to the maternity unit’s birthing rooms and the obstetric theatre for easy
transfer of the baby in case of complications
There should be easy access from the postnatal area to the neonatal unit, so that the mother can easily see
her baby
Relationships with external facilities
Where there are paediatric surgical services on site, neonatal units should have direct access to the paediatric
operating theatres.
Avoid direct sun into the Nurseries to minimise the need for critical sun protection.
Care must be taken to avoid placing the actual nurseries adjacent to noise sources such as plant rooms, lifts
and public lobbies.
Internal relationships within the neonatal unit
Key relationships within the neonatal unit include:
Clinical support areas should be as close as possible to clinical care areas. Such support facilities include the
near-patient testing laboratory, pharmacy, equipment storage, milk storage, clean and dirty linen store.
Family access is required to the waiting area, interview rooms, support services (for example social work and
community neonatal nursing) and recreational facilities.
The attending consultant’s office should be located within the neonatal unit.
On-call accommodation should be located in the neonatal unit or immediately adjacent to it.
Consultant and research offices can be located further away from the clinical care area.
In larger units, the milk kitchen should have an associated, separate store.
The milk expression room should be located close to the milk kitchen.
Family-centred care
Parents are encouraged to visit and stay with, handle and care for their babies, and high priority should be
given to the needs of the family. This is especially important when a baby is moved for ongoing intensive care.
Accommodation for families should be within easy reach of the neonatal unit, including family rooms,
bathrooms, basic self-catering facilities and a play area for siblings of infants receiving care.
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
7
Kangaroo Mother care (KMC) includes “rooming in” facilities, where parents can look after their baby/babies
with supervision from midwives and neonatal professionals for up to two weeks, prior to transfer home. This
guidance assumes the following:
the mother requires further care and support, which takes place in multi-bed bays generally
associated with post-natal beds or
the focus is on the neonate who has been unwell, and care takes place in parent rooms generally
associated with the neonatal unit.
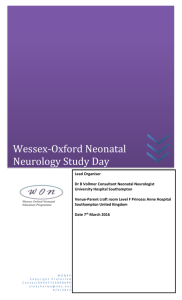
Functional Relationships - Maternity and Neonatal
POST NATAL WARD
Entrance & Exit
Rooming in
Delivery Suite
Well baby
Nursery
counseling
Public waiting
Kangaroo mother care
KMC
Access Control
SISTER’S
OFFICE
ISOLATION
NEONATAL
General Care
NEONATAL
NURSES
SLUICE
STATION
HIGH CARE
STAFF
Milk Kitchen
NEONATAL
ICU
Storage
Clean Utility
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
8
Departmental Functional relationships
Post Natal Ward
Kangaroo Care
Area
Infection Control
Neonatal Unit
Birthing
Suite
Mortuary
Obstetric theatre
floor
Located within the same building
Located on same floor
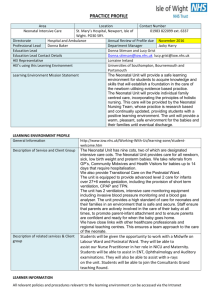
Patient Flow: Neonates
Neonatal Unit
Obstetric theatre
BIRTHING UNIT
Home or
Referral
Well baby
Post Natal Ward
“Rooming in”
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
9
Flow of the maternity and neonatal:
Antenatal
ward
Entrance
Assessment
Antenatal ward
Entrance,
Admission,
Aassessment area
Delivery suite
Neonatal resuscitation area
Post Caesarian section cubicle
Post natal cubicles
Well baby nursery
Neonatal nursery for small and sick babies
All the support services
Staff facilities
Service facilities - storage, ablutions, sluice room etc
Patient facilities – counseling rooms
Admissions
Neonatal
Resuscitation
Delivery
suite
Neonatal
nursery
Well baby
nursery
Post Natal
ward
Spacing
Diagram of cot spacing
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
10
SERVICES
NICU
HIGH CARE
Power Outlets
POST
natal
2
16
12
Oxygen
Medical Air
Vacuum
Emergency call
Baby bath
1
0
1
yes
y
3
3
2
yes
n
2
2
1
yes
n
WHB
Service Provision
Ceiling
Service Provision
Wall
Space
750 incubator
AND BEDS
1/6
1/4
Pendant
1/6
NURSERY
intermediate
2 electrical plug
1 oxygen
None
1 per bed
yes
Work surface and
sink
1/6
Paediatrics
Bed & cots
Same as R158
Paediatric ICU
& HC
16 UPS
isolated
power supply
yes
y
yes
y
1/6
1/6
1200 wall to
bedside
Bed 1050
1900 between beds
2400 foot to foot of
bed
4500 square
provision
wall
750 to wall
2400 between cots
1200 cot to wall
2700 foot to foot
750 to wall
2400 between cots
1200 cot to wall
2700 foot to foot
600 to wall
2400 between cots
900 cot to wall
2000 foot to foot
Design and Planning
Rooming-in facilities:
Rooming-in to be considered the Norm on all post natal wards
1,5m space between beds on the post natal ward to accommodate the bassinette for the well babies to sleep
next to their mothers
CLINICAL AREA
The Nursery Component is comprised of:
Well baby area in the post natal ward (separate to the neonatal unit
The neonatal unit comprising:
A Neonatal ICU
A Neonatal High Care
A Neonatal General care
Isolation ward
Standard components in the neonatal nursery
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
11
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
o
Clean Utility
Cleaners closet
Doctors office
Dirty Utility
Overnight facility- doctor
Sisters Office
Store – Clean linen
Store – Equipment
Store – Surgical
Store - Sundries
Store medical
Staff Change
Staff Rest
Staff Toilet
Sisters Office
Central Nurses Station
Stores
Staff facilities
Dirty Utility
Sluice
Clean Utility
Doctors office
Overnight facility- doctor
Milk expressing area
Ward kitchen
Ward laboratory
Clinical technologist office (standard office space)
Well Baby Nursery
DESCRIPTION
A nursery catering for newborn ‘well babies’ where the neonatal nursery is a component of the maternity
wards. The Well Baby Nursery will provide facilities for the care of well babies away from their mother's bed
area and for the following functions:
This is an integral part of the post natal component of the ward. It needs to cater for well babies and allow for
observations, procedures, phototherapy and bathing.
SPACE
A Well Baby Nursery in a hospital must have:
A minimum floor area of 1.5m² per bed/cot
Minimum area of 35m²
LOCATION
To be located within the nursery unit, usually behind or next to the nurses station, adjacent to both the
nurses’ station and the waiting area with a viewing window between the waiting and well baby nursery to
display the newborns at specified times to visitors in the waiting area.
The Well Baby Nursery will be located with ready access to Maternity inpatient bedrooms used for post-natal
care
SERVICES
Heated to an ambient temperature of around 26o C
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
12
A baby bath with adjacent work surface- Bathing of babies using controlled temperature
water. Baby bath -1 per 10 cots- baby bath with adjacent work surface
Two sets of service points with oxygen, suction and four electrical outlets each
Resuscitation including oxygen, medical air and suction
Weighing of babies
Use of staff assistance call and emergency call.
Hands free wash hand basin with elbow action taps – 1 per 4 cots
Oxygen points
– 1 per 2 beds
Suction
– 1 per 2 cots
Electrical outlets
– 4 per 2 cots
Lighting – adjustable from 10 – 600 lux
CONSIDERATIONS:
The Well baby unit will require the following:
Clear glazed glass partitions for easy observation of the babies with direct view from the
nurse’s station into the nursery,
Heated to an ambient temperature of 26 degrees C,
Space for a resuscitation unit and four basinets
Isolation unit attached,
An intercom through to the waiting area for visitors to request a specific baby be shown
at the viewing
Window,
Natural and artificial lighting, colouring corrected to natural,
General comfort air-conditioning,
An emergency call system,
A dedicated area within or adjacent to the nursery to allow easy examination and
changing of the baby, and storage of necessary linen and equipment,
An area within the Nursery that can be made available for stabilisationprior to transport
by a transport team. Changing, cleaning and drying of babies
Feeding of babies in comfortable chairs
Parent and staff education
T assist sleeping of babies in daytime using partial blackout curtains
Storage of supplies such as nappies, towels, creams and powders
Waste and dirty linen disposal
Work surface to change babies nappies etc. Smooth, non porous surface, easy to clean.
Waste disposal bins
Neonatal Nursery
This must form an independent component within the maternity ward with a KMC unit, an isolation cubicle
and patient area with general and high care beds.
Requirements of this unit are:
Single access point .
The entrance is to be access controlled
Support services separated from patient area by double doors
Hand basin on entry to the unit
The entire unit must have ambient temperature of around 26o C
ENTRANCE INTO THE NURSERY AREA
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
13
The Entrance into the nursery area requires access control connected to the Sisters Office and Nurses Station.
Strict Security Control of the Nursery is essential.
LOCATION AND RELATIONSHIPS
The Entrance should be adjacent to the Sisters Office which shall have a full view of persons entering and
exiting the unit.
The Entrance shall open directly into the Nurses Station area and be in full view of that area.
FLOW:
Entrance to support services area
KMC unit off the support services
Central Sister-in-charge’s office:
o to control access to nursery & KMC unit
o allow observation of isolation cubicle & patient area
Isolation cubicle
Patient area
NURSERY
Minimum of 4 beds – 50% high care and 50% general beds
Services for high care beds - oxygen, medical air, suction and 10 electrical points per bed
Services for standard beds – oxygen, suction and two electrical points per two beds
Hands-free basin – 1 per unit or every six beds
Baby bath – 1 per unit or every ten beds
ISOLATION UNIT
1 bed per unit
Minimum space of 6 m2 per cubicle
Hands-free basin at entrance
Serviced with oxygen, medical air, suction and 10 electrical points
Nurses work station with a view of all beds
SUPPORT SERVICES
Sister’s office
Staff room with en-suite ablution
Counseling room
Multipurpose storeroom
Equipment storeroom
Small kitchen
Toilet - Public/Disabled
Counselling/Interview Room
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
14
The norms of the physical requirements for a stand alone regional or tertiary level neonatal nursery, based on
the R158, KwaZulu-Natal Recommended Guidelines for Infection Control in Newborn Care and 7th Consensus
Conference on Newborn ICU Design, are detailed below.
General
ICU (5)
High Care (7)
Bed space
1.5m2
5m2
5m2
Wall length at head of bed
1m
2m
2m
Space between beds
1m
2.4m
2m
Aisle width
1.5m
2m
2m
Patient Area:
1
Space allocation:
Minimum of 4 beds – 50% high care and 50% general beds
2
Services:
Hands free basins
1 per unit / 6 cots
Baby bath & work surface
1 per unit / 10 beds
Oxygen point
1:2
Medical air
3
2
2
1
1
Suction
1:2
2
2
Electrical point
2:1
10
12
Lighting - ambient
Adjustable range 10 – 600 lux
Lighting - procedural
2000 lux spot ICU/HCU bed
Nurses Station
1 per 16 beds. View to all patients
Isolation Room:
Beds per cubicle
1 bed per unit
Minimum space
8m2
Services
Services with oxygen, medical air, suction and 10 electrical points
Hands free basin at entrance
4
Kangaroo Mother Care Unit
Accommodation
Maximum 6 patients per bed unit
Miniumu 7.5m² per bed
Lounge/Dining area
10m²/5 mothers
Ablutions
1 bath / shower per 12 mothers
1 toilet & basin per 7 mothers
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
15
5
6
Patient support area:
Counselling room
6 – 8m2
Consulting room
6 – 8m2, hands-free basin
Day room, en-suite toilet
To accommodate 6 people
Support areas:
Clean utility rooms:
Sundries store
Linen & haberdashery store
Pharmaceutical store
5m2, work surface & hand basin
5m2, shelving
Shelves & medicines cupboard
Equipment cleaning room
Double bowl sink & drying racks
Equipment store
Open shelving under counter top
O2, medical air, vacuum & multiple electrical points
Dirty utility room
5m2 for stand alone unit
7m2 if combined with cleaner’s room
Hand basin, sluice sink & drying racks
Cleaner’s room
Ward kitchen
Shelves, hand basin, low level sink & slop hopper
4m2 increasing by 1,5m2 per 10 beds
Single bowl sink, work surface, storage space & hand basin
Ward laboratory
Clinical technologist office
7
Hand basin, work surface
Hand basin, work surface, electrical points, O2, medical air & vacuum
Staff support area:
Sister’s office
6 – 8m2, hands-free basin
Staff locker room
Tea room / lounge
Ablutions
Doctor’s office
On call suite
1 per 36 beds
6 – 8m2
1 bedroom per doctor
En-suite bathroom
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
16
Non standard spaces within the neonatal unit:
Neonatal Bay General
DESCRIPTION AND FUNCTION
A single bay for the care of well babies away from their mothers bed area where the new born babies are
observed and stabilised after birth or have Phototherapy
The neonatal bay shall be a minimum of 5 m2, which includes a circulation area of 1 m between bays.
LOCATION AND RELATIONSHIPS
The Neonatal Bay – General Care will be located within the Neonatal Nursery.
The Neonatal Nursery will be located with ready access to Maternity inpatient bedrooms used for post-natal
care.
CONSIDERATIONS
A hands free handwash basin should be provided for each four neonatal bays – general care.
Neonatal Bay – Intensive Care
DESCRIPTION AND FUNCTION
A single bay for neonates requiring intensive care nursing and medical treatment. The bay (or room) will
include provisions for charting and storage.
The neonatal bay/room – ICU shall be a minimum of 12m2. In multibed rooms a minimum of 2.4 metres is
required between infants beds, with an aisle of 2 metres between beds facing each other.
LOCATION AND RELATIONSHIPS
The neonatal bay – ICU will be located in Neonatal/ special care area, which will have ready access to the
maternity inpatient unit, obstetric unit, operating unit, emergency unit and pathology unit.
CONSIDERATIONS
A staff clinical hands free handwash basin is required in close proximity to each neonatal bay – ICU.
Each bay shall be within 6 metres of a handwash basin.
Neonatal Bay – High Care
DESCRIPTION AND FUNCTION
A single bay for neonates requiring special care nursing and medical treatment. The bay will include provisions
for charting and storage.
The neonatal bay/room -HC shall be a minimum of 10 m2. In multi-bed rooms a minimum of 2 metres is
required between infants beds, with an aisle of 2 metres between beds facing each other.
LOCATION AND RELATIONSHIPS
The neonatal bay special care will be located within the intensive care unit – neonatal/special care, which will
have ready access to the maternity inpatient unit, obstetric unit, operating unit, emergency unit and pathology
unit.
CONSIDERATIONS
A staff hands free clinical handwash basin is required in close proximity to each neonatal bay – special care
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
17
Neonatal - Isolation Room
DESCRIPTION AND FUNCTION
Isolation Rooms are used to isolate patients with known infectious conditions or to protect patients from
infection. They may be positive pressure or negative pressure but not both.
LOCATION AND RELATIONSHIPS
The Isolation Room requires facilities to bath the new born.
Where the Isolation Room is pressurised, an Anteroom or Airlock will be required for pressure stabilisation.
One Neonatal isolation room per 36 post natal beds
Minimum area
8m²
Minimum wall length of cubicle
2.4m
1 cot per cubicle
SERVICES
Services to be provided in wall
Hand wash basin with elbow taps and gooseneck outlet in each room with tiles above, mirror, soap dispenser
and paper towel dispenser
1 per unit
Oxygen point
2
Medical Air
1
Suction
2
15 Amp electrical plugs
10
Air conditioning
Air pressure in ward unit to be Negative
pressure for contagiousdiseased patients and Positive pressure for immune compromised
patients where patient requiresprotection
CONSIDERATIONS
All surfaces must be impervious and designed for easy cleaning
Glazed, clear panels to allow for observation into the room
Milk Kitchen
DESCRIPTION
This is to be central to and shared by all the nurseries. To be closest to the neonatal nursery
Required for hospitals with more than 20 neonatal and paediatric beds
LOCATION
Ideally situated in or near CSSD with access to an autoclave or Close to neonatal ward if the kitchen has its own
autoclave
FLOW
Dirty bottles received
Bottles cleaned and autoclaved
New feeds made up and bottled
Bottles dispatched to wards
REQUIREMENTS:
“Dirty” area - to clean feeding utensils: Minimum 9m²
Hands free basin,
work surface,
double sink & bottle cleaner,
sufficient work surface for “3-bowl” cleaning process,
3 electrical plug point
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
18
Storage space Work surface, storage shelves or cupboards
“Clean” area to prepare feeds: Minimum 9m²
Hands free basin,
work surfaces for sterile & unsterile purposes,
3 electrical points (fridge, urn & mixers),
double sink
Kangaroo Mother Care Unit (KMC)
DESCRIPTION
Unit where mother and child room together
Minimum of 2 beds
En-suite ablutions
Day room / lounge
LOCATION
Access from support area of nursery
Within close walking distance of the neonatal ward
BED ACCOMMODATION
Maximum 6 patients / cubicle
minimum 7.5m2 / bed
Close to support area
Minimum of 2 beds
ABLUTIONS
1 bath/shower per 6 mothers
1 toilet & wash hand basin per 6 mothers
Standard Components - KMC
Bath
Cleaner’s Room
Clean Utility
Day Room
Dirty Utility (Sluice)
Kitchen
Store – Clean Linen
Store - General
Shower-Patient
Toilet-Patient
Waste Disposal
Design Considerations
SAFETY
There must be adequate space around the cot to enable staff to work safely - particularly in an emergency and
for easy access for equipment such as x-ray and ultrasound units and a mother’s bed.
SECURITY
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
19
The security system should protect the physical safety of infants, families and staff in the Unit and in particular
should minimise any risk of infant abduction.
Babies born in hospital should be cared for in a secure environment to which access is restricted. Single
controlled entry for the public and visitors.
A robust and reliable baby security system should be enforced. Consider closed circuit television with phone or
intercom for after-hours access.
An effective system of staff identification is essential. Separate staff entry and entry for goods and waste
removal - if provided -must be by smart card access or similar.
Emergency exits to be alarmed.
Strict criteria for the labelling and security of the newborn infant are essential - Baby security tag system.
Ready access to duress alarms for staff.
Security systems should not compromise the ability of staff to carry out their work or to respond to
emergencies when required.
ACCESS
EXTERNAL
- Drop off and parking for parents
- Access to long-term parking (regional families)
- Access for wheelchairs, prams and strollers
- Easy transfer of babies to the Operating Suite
- After hours - but separate - access for parents / staff
- Bed/trolley access for mothers from postnatal wards
- Keyed lift to Helipad or equivalent
- Ambulance
- Outside area readily accessible from the Unit to give families relief from the clinical environment
INTERNAL
Balanced with the need for security is the issue of access. All doors between the maternity area and the
neonatal unit, and also those within the neonatal unit, should be designed to maximise convenience as well as
safety and security. If automatically locking magnetic doors are to be used, consideration should be given to
difficulties that may arise in wheeling incubators/cots from room to room in an emergency when the security
doors have locked down.
Access must be ensured for mothers on trolleys or in wheelchairs. Widths of doors, corridors and corners
should be considered so that mothers have access to all clinical areas
Must allow access and ease of movement for an x-ray or ultrasound unit, a mother in a bed or on a trolley.
Minimise exits - public, staff, goods entry & waste removal.
It is worthwhile calculating the widest and longest object that may travel along the corridors. This may be a
mother in a bed who is visiting her baby or a retrieval incubator plus staff. This can ensure that the journey can
be safely accomplished in the shortest and most direct route and can facilitate decisions as to which way
corridor doors should open, and whether they open automatically or by push-button or electronic access. Such
travel
patterns may inform the eventual design of the Unit and its connections with the rest of the hospital including
evacuation plans
NEONATAL CARE ENVIRONMENT
The environment in every neonatal area needs to be completely controllable in terms of noise, light, smell,
view etc.
Sound levels should be controlled and kept below 40 db (womb-like level). This means controlling airconditioning noise, telephone and paging system sounders and all other extraneous background noise.
Stainless steel sinks and troughs can be very noisy; where used, care should be taken to avoid high water flow
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
20
that results in excessive noise. Waste bins should be foot-operated with soft-close tops. Consideration should
also be given to noise levels from floor coverings, door closers etc. This needs to be balanced with the need to
minimise HCAIs. Sound-monitoring equipment may help to maintain low noise levels.
Similarly, the visual environment should be fully controllable and able to be blacked out. In intensive care cot
areas, it should ideally be possible to control lighting to individual babies
Natural light should be provided to all clinical areas, quiet rooms and parents’ bedrooms. Babies’ cots should
be positioned no closer than 600 mm from any external window. Radiant heat gain should be minimised with
shading to prevent overheating. Full consideration should also be given to the need for family privacy
Other considerations include:
- temperature and humidity controland
- infection control.
LIGHTING IN CLINICAL AREAS
Artificial lighting should be chosen very carefully. All artificial lighting should be indirect, except for lights
needed for procedures, and it is preferable that each light should be individually controlled. This is particularly
important in special care areas where a relatively well child can sleep in darkness even when another infant in
the same room is being examined. The ability to achieve darkness is very important, not just for the sleeping
infant but also for procedures such as echocardiography and chest transillumination. Window shading is
essential, and blinds should be provided with privacy glass screen type or vertical cleanable type
All clinical areas should have controlled natural lighting for the development of circadian rhythms in the infants
and to enhance staff performance and wellbeing.
Direct overhead ambient lighting in the infant care space must be avoided as well as direct lighting outside the
area that may be in the infant’s line of sight to minimise danger or damage to the developing retina, visual
pathways and developing brain.
Lights should be angled or designed to reduce reflection off the incubator canopy.
Light levels should be no brighter than needed to complete a task, and individualized lighting should be
available at each baby station.
Reduced lighting also has been shown to significantly reduce conversation levels among staff, the primary
contributor to noise in an intensive care unit.
Thus the infant care space should have three separate light sources and controls:
- General room ambient lighting - controlled by dimmer.
- Individual work space lighting - not direct on infant with controls to allow immediate darkening of any cot
position to permit trans illuminance. (The passing of a light through the walls of a body part or organ to
facilitate medical inspection).
- Observation/procedure light for every infant space.
Lighting must be colour-corrected to natural lighting.
Ambient lighting levels in cot bays should be adjustable, through a range of at least 100 to 600 lux as measured
at each bedside.
Recommendations for specific tasks and interiors
PROCEDURE LIGHTS
Each NICU cot must have a local light for emergency use, observation and procedures. This light should be
appropriate in intensity and area of focus and may be adjustable.
High Dependency Level 2 cots require 1 procedure light per cot
Low Dependency Level 2 cots require access to 1 mobile procedure light per work area
Lights must be shaded to minimise shadow and glare to adjoining cots.
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
21
TEMPERATURE CONTROL
- Air temperature of 22-26°C (72-78°F)
- Relative humidity of 30-60%
- A minimum of six air-changes per hour
- Minimising of draughts on or near infant beds
- Filtration of ventilation air at least 90% efficient.”
Individual thermostats.
Air-conditioning / ventilation outlets located with care to avoid draughts over Essential - both visual and
speech.
INTERIOR DESIGN
“Color selection relative to infants is largely inconsequential, (she says) because of their lack of visual
perception, but with regard to adults, studies have indicated persons in high anxiety situations prefer pastels
rather than saturated colors. Common sense, dictates that colourr schemes should be subdued so they don't
interfere with accurate reading of the infants' skin colour.
ACOUSTICS
“Numerous studies identify noise as a primary stressor for infants, patients and staff of health care facilities, with infants
particularly disoriented by noise because their hearing is still immature, … Noise can prevent an infant
from reaping the developmental benefits of sleep, but noise can be reduce d through acoustic and configuration
modifications to the facility and modifications in staff behaviour through educational programs. However,
some forms of noise, such as music, have been shown to be effective in reducing stress in infants by reducing cortisone
levels in the brain that areassociated with stress”
MardelleShepley, Neonatal Intensive Care Unit Designs are critical to infant health, June, 2005.
Ambient (i.e. background) noise levels should not exceed an hourly Leq 40-45 dB(A)
Noise control measures may include:
- Acoustic ceiling tiles with a noise reduction co-efficient of at least 0.9. (Maydepend on local infection control policies)
- Double glazing
- Flooring with sound-absorbing qualities
- Duct baffles
- Walls of sound absorbing materials
- Special acoustic insulation for noise-producing equipment at the cotside.
Noise output should be a criterion when selecting equipment
INFECTION CONTROL
the importance of good infection control practices in the newborn environment cannot be overstressed.
Clinical handbasins will be provided at a ratio of 1:2 in intensive care and 1:4 special care cots and staff must not have to
travel more than 6m from cot to basin.
Isolation rooms will be provided for babies with known infections
CLINCAL HANDBASINS
Clinical handbasins should be provided at a ratio of 1:2 in intensive care and 1:4 in the special care nursery and staff must
not have to travel more than 6m from cot to basin. At least one basin must be available for children
and people in wheelchairs.
The space occupied by the basins is additional to the size of the cot bay.
Design requirements:
- hands-free operation is preferred;
- water flow must not fall directly into the drain outlet;
- sized to avoid splashing and splash-back from the drain;
- no pooling allowed at the bottom of the basin;
- pictorial hand-washing instructions at every sink.
References and Further Reading
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
22
Design Guidelines for Neonatal Units for Australia and New Zealand. First
Draft - 17th May 2004, Dr. Neil Roy, Divisional Director (Medical) - Neonatal
Services, Royal Women’s Hospital, Melbourne and Dr. Carl Kuschel,
Director of Neonatal Unit, National Women’s Hospital, Auckland, New
Zealand for the Australia & New Zealand Neonatal Network.
A Review of Neonatal Intensive Care Provision in New Zealand, Ministry of
Health, February 2004.
HPU 390 - Intensive Care-Neonatal / Special Care Nursery, Department of
Human Services, Victoria, November 2004.
“Designing a Neonatal Unit”. Report for the British Association of Perinatal
Medicine, May 2004.
Health Canada. Family-Centred Maternity and Newborn Care: National
Guidelines, Minister of Public Works and Government Services, Ottawa,
2000. (Chapter 10, Facilities and Equipment).
Standards for Hospitals Providing Neonatal Intensive and High Dependency
Care, 2nd edition, British Association of Perinatal Medicine, December 2001.
Recommended Standards for Newborn ICU Design, Report of the Fifth
Consensus Conference on Newborn ICU Design, January 2002, Clearwater
Beach, Florida, Committee to Establish Recommended Standards for
Newborn ICU Design, Robert D. White, MD, Chairperson, Memorial
Hospital, South Bend, Indiana. Sourced AEST 22/08/2005
Mardelle Shipley. Neonatal intensive care unit designs are critical to infant
health”, Jun 17, 2005, 03:32. Sourced AEST 10/08/2005
“A Single-Room NICU-The Next Generation Evolution in the Design of
Neonatal Intensive Care Unit, American Institute of Architects. AEST
10/08/2005
United Nations Convention on the Rights of the Child, Article 24.
et al references 1987–2008:
American Academy of Pediatrics, Levels of Neonatal Care, Committee
on
Fetus and Newborn, Pediatrics, 2004; 114;1341-1347.
Neonatal Intensive Care Unit - Design Brief, Child Health, July 2002, Capital
and Coast District Health Board, Wellington Hospital, New Zealand.
Neonatal Services - Functional Brief, Royal Women’s Hospital, Melbourne,
2004.
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
23
Graven SN and Browne JV.Sensory development in the fetus, neonate, and
infant: Introduction and overview. CNS-BC Newborn & Infant Nursing
Reviews , December 2008 Volume 8, Number 4, www.nainr.com
Graven SN. Impact of the environment on development in Report of Fourth
Annual Ross Planning Associates Symposium, 1987.
Graven SN, Bowen Jr FW, Brooten D et al. The highrisk infant
environment.Part 1.The role of the neonatal intensive care unit in the
outcome of highrisk infants.J Perinatol. 12(2):164–172, 1992.
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
24
Newborn Individualized Developmental Care and Assessment Program SLL LIGHTING GUIDE 2:
Hospitals and health care
Graven SN. Clinical research data illuminating the relationship between the buildings
physical environment and patient medical outcomes.J. Healthc. Des. 9:1519,
1997.
Lister JJ, Graven SN, HnathChisolm T and Eaton C. Effects of early sensory
environment and preterm birth on auditory processing abilities.Acad.,
Pediat.Soc., 2003.
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides:10 June 2012
Paediatrics & Neonatology units [DISCUSSION DRAFT 1]
25
PART C – Accommodation schedules
Accommodation Schedule - Neonatal Unit
NEONATAL NURSERY– ENTRANCE AREA
ROOM
Standard
Component
Main Entrance/Reception
Quantity
Area Each
m²
Total
m²
x
1
5
5
Visitors Waiting
x
1
10
10
Counseling Room
x
1
9
9
Toilet - Public
x
2
4
8
Toilet-Disabled
x
1
5
5
1
4
4
4
9
36
Entrance into Nursery
Non Standard
Component
x
NEONATAL NURSERY – NURSERY AREA
Isolation Room
x
Neonatal Bay – General
x
16
5
80
Neonatal Bay – Intensive Care
x
4
12
48
Neonatal Bay – SpecialCare (HC)
x
14
10
140
Nurses Station
x
1
10
10
Bay - Handwashing
x
19
1
19
Bay – Resuscitation Trolley
x
3
1
3
x
1
45
45
Non Standard
Component
Quantity
Area Each
m²
Total
m²
2
12
24
1
16
16
Well baby Nursery (18 basinetts)
NEONATAL NURSERY – SHARED AREAS
ROOM
Standard
Component
Doctor’s Office
x
Central Nurse’s Station
x
Sister’s Office
x
1
12
12
Staff Toilet
x
1
2
2
Staff Restroom
x
1
20
20
Staff Change
x
1
12
12
Bay - Handwashing
x
1
1
10
Cleaners’ Room
x
1
6
6
Clean Utility
x
1
6
6
Dirty Utility
x
1
9
9
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides: 1 February 2012
Paediatrics & Neonatalogy Units [DISCUSSION DRAFT 1]
26
Overnight Stay - Doctor
x
1
9
9
Store - Clean Linen
x
1
6
6
Store – General
x
1
9
9
Store - Surgical
x
1
6
6
Waste Disposal
x
1
4
4
Non Standard
Component
Quantity
Area Each
m²
Total
m²
Receiving area
x
1
4
4
Dirty Area
x
1
9
9
Clean Preparation area
x
1
9
9
Store
x
1
12
12
Dispatching area
x
1
4
4
Non Standard
Component
Quantity
Area Each
m²
60
12
6
1
6
6
36
9
9
4
6
9
2
4
Total
m²
120
12
6
4
6
6
36
9
9
8
6
9
8
4
MILK KITCHEN
ROOM
Standard
Component
KANGAROO MOTHER CARE– SCHEDULE OF AREAS
ROOM
Standard
Component
6 bed unit
x
Isolation Room
x
Bath
Bay - Handwashing
x
Cleaners’ Room
x
Clean Utility
x
Day Room
x
Dirty Utility
x
Kitchen
x
Shower-Patient
x
Store - Clean Linen
x
Store – General
x
Toilet-Patient
x
Waste Disposal
x
x
2
1
1
4
1
1
1
1
1
2
1
1
4
1
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides: 1 February 2012
Paediatrics & Neonatalogy Units [DISCUSSION DRAFT 1]
27
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides: 1 February 2012
Paediatrics & Neonatalogy Units [DISCUSSION DRAFT 1]
28
PART D – Room data
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides: 1 February 2012
Paediatrics & Neonatalogy Units [DISCUSSION DRAFT 1]
29
LIST OF ABBREVIATIONS
ENT
Ear nose and throat
HIG
Hospital Infrastructure Grant
HRG
Hospital Revitalisation Grant
IUSS
Infrastructure Unit Systems Support
NDoH
National Department of Health
OoM
Order of Magnitude
PMIS
Project Management Information System
PMSU
Project Management Support Unit
RC
Recommendation Committee
INFRASTRUCTUREUNITSUPPORTSYSTEMS(IUSS)PROJECT
Health Facility Guides: 1 February 2012
Paediatrics & Neonatalogy Units [DISCUSSION DRAFT 1]
30