immunization record - Samford University
advertisement

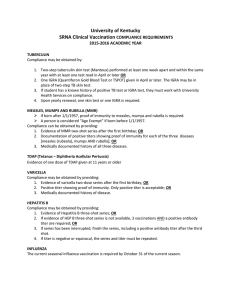
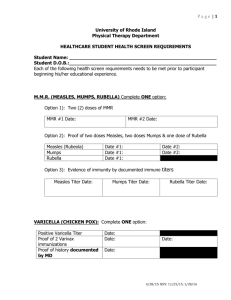
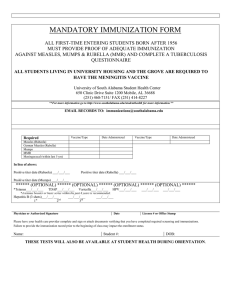
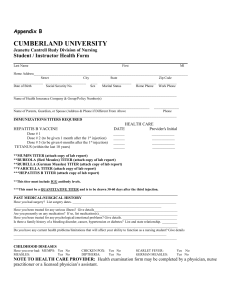
IMMUNIZATION RECORD Keep a paper or electronic copy for your records. Required of all McWhorter Pharmacy Students Immunization Status is held to the standards for healthcare professionals. Name: _____________________________________________________________________________ SID: __ __ __ __ __ __ __ __ __ Last First MI Cell Phone # ________________________________ Preferred name Date of Birth: ____/____/________ Entering: _____ Year MEASLES / MUMPS/ RUBELLA (MMR) All entering students born after January 1, 1957 must have A or B: A: Documentation of two doses of MEASLES/MUMPS/RUBELLA (MMR) vaccine First dose administered since January 1, 1968 and on or after the first birthday Second dose administered at least 28 days after the first dose B: Documentation of immunity by blood test (titer) demonstrating protective antibody levels to measles, mumps and rubella. #1 M.M.R (Measles,Mumps,Rubella) #2 Date of Titer Measles ____/_____/_____ _____/____/_____ Attach copy of report _____/_______/______ Date of Titer Mumps Attach copy of report _____/_______/______ Date of Titer Rubella Attach copy of report ______/______/______ HEPATITIS B If a vaccination series has not previously been completed, the first dose must be administered prior to the first week of class attendance. Completion of the full series is required by March 1st of the P1 year. Documentation of immunity by a blood test (titer) is required once series is completed or in lieu of vaccinations. #1 #2 _____/_____/_____ Date of Titer #3 _____/_____/_____ _____/_____/_____ TETANUS DIPTHERIA PERTUSIS (Tdap) Tdap is required ( one-time vaccination) Attach copy of report Hepatitis B Surface Antibody _____/_____/_____ MENINGOCACCAL QUADRIVALENT Required of all students living in University housing. Tdap If Tdap over 10 years ago, booster required. Tetanus/diphtheria date: _____/______/_______ Td Students <21 years must have a dose of conjugate vaccine at > 16 years of age _____/______/_______ ___/____/___ VARICELLA (Chickenpox) Documentation of two doses of vaccine at least 4 weeks apart. The first dose must be administered prior to the first week of class attendance. Documentation of immunity by blood test (titer) or date of disease is acceptable in lieu of vaccine administration dates. #1 #2 _____/_____/_______ Date of Titer _____/_____/_______ Varicella AB, IgG _____/_____/______ Attach copy of titer report Date of Disease _____/_____/______ TWO-STEP TUBERCULIN SKIN TEST (Mantoux PPD) Skin tests should be 1-3 weeks apart (must be within 12 months prior to first day. ) 1. Initial Tuberculin Skin Test (TST) nd 2 Tuberculin Skin Test (TST) 2. Date Placed: _____/____/_____ Date Read: ____/_____/_____ Results: (mm induration) __________________ Date Placed: _____/____/_____ Date Read: ____/_____/_____ Results: (mm induration) __________________ Chest X-ray required if TST is positive OR if history of positive TST in the past. Chest X-ray must have been within 12 months prior to first day of class. Date of Chest X-Ray: _________________ Results: (*attach copy of test results or report ) THIS RECORD MUST BE SIGNED BY A HEALTH CARE PROVIDER (Health Department stamp acceptable) MD/PA/NP/RN Signature: _________________________________________________ Print Name: ________________________________________________ Phone: ( Date: _________________________ ) _______________________________ Address: ____________________________________________________________________________________________________ RETURN ORIGINAL FORM TO: SUBMIT COPY TO: Samford University Health Services, 800 Lakeshore Dr., Birmingham, AL 35229 McWhorter School of Pharmacy, Ingalls 252, 800 Lakeshore Dr., Birmingham, AL 35229