Tracthe_UTI_Antibiotics_12.09.09
advertisement

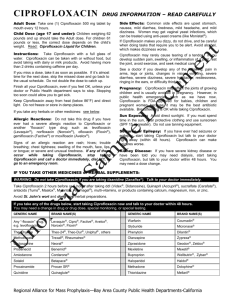
Class Drug Trimethoprim/Sulfamethoxazole MOA –Blocks folic acid synthesis -SMX: sel toxic to bacteria b/c mammalian cells lack dihydropteroate synthetase Spectrum Flurinated quinolones Blocks the uncoiling of DNA by preventing the action of topoisomerase II and IV (DNA gyrase) - CIDAL Blks topoisomerase II & IV Damage DNA, bacteria convert to highly reactive intermediates Converted to formaldehyde & ammonia in ACID environment only -cidal G- UTI Urinary tract antiseptics Ciprofloxacin Norfloxacin Nalidixic acid Nitrofurantoin Methenamine Resistance Dist/Elim -Staic & cidal G-/+ Broad spectrum Mutation of binding site on topoisomerase -pseudomonas -cidal limited Conc in the urine Conc in the urine, contraindicated w/renal failure Everywhere, but only converted in acid environ. (urine!) 1. Summary a. Multiple drug treatments for urinary infections i. Empirical treatment typically involves Fluoroquinolone (Ciprofloxacin), Trimthoprim/Sulfamethoxazole and/or Nitrofurantoin ii. Drugs that are not excreted in their active form in urine are erythromycin, Chloramphenicol, Rifampin iii. Drugs with known toxicity in pregnancy are tetracyclines (brown teeth) and sulfa drugs 1. Suspect that there is toxicity (from animal studies) for trimethoprim, clarithromycin, ciprofloxacin, fluconazole, miconazole, terconazole, isoniazid, rifampin and mebendazole 2. No known toxicity (in pregnancy) for amoxicillin, ampicillin, dicloxicillin, nitrofurantoin, metronidazole, Cephalosporins, clindamycin, erythromycin, azithromycin, famciclovir, acyclovir, clotrimazole 3. No fetal harm from Nystatin b. Emphasize mechanism of action for: i. nitrofurantoin – 1. damage to DNA by reactive metabolites 2. Secreted into renal tubules to have a selective urinary antiseptic effect ii. Nalidixic Acid 1. Quinoloine affecting DNA gyrase 2. Similar concentration mechanism iii. Methenamine 1. Generates formaldehyde in an acidic environment c. Know that dose adjustments relate to creatinine clearance if drug is cleared by kidney and the effect of age on creatinine clearance d. Know generalities about time- and concentration-dependent killing Practice Questions: 1. 2. 3. The key concept behind the effectiveness of urinary tract antiseptics is_____________. If a patient as decreased renal function, should you change antibiotic dosing? What are your options for dosing changes? Match the UTI antibiotic with the mechanism of action: A. Trimeth/Sulfmeth. B. Ciprofloxacin C. Nalidixic acid D. Nitrofurantoin E. Methenamine MOA: 1. blocks topoisomerase II & IV (2 drugs) 2. blocks folate metabolism 3. converted to formaldehyde & ammonia in acidic environment 4. damages DNA, bacteria convert it to highly reactive intermediates 4. Patient present in clinic with UTI. Empirically, what three drug classes could you use to treat the patient? 5. A pregnant patient presents in clinic with a UTI. What drug/drug classes would you avoid using because they are Class D teratogens (2)? What teratogenic classes do the other options belong to? A. Nystatin B. tetracyclines C. sulfa drugs D. nitrofurantoin E. ciprofloxacin Answers: 1. they are concentrated in the urine. 2. Yes, either reduce dose or change time interval between dosing. 3. A, 2; B, 1, C, 1; D, 4; E, 3 4. T/S, fluorinated quinolones, urinary tract antiseptics. 5. Class D = B &C, A, Nystatin is class A (not harmful); D, nitrofurantoin is class B; E, Ciprofloxacin is class C.