Name: DUE DATE: Cardiovascular and Respiratory Systems
advertisement

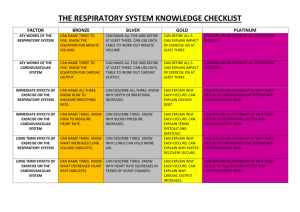
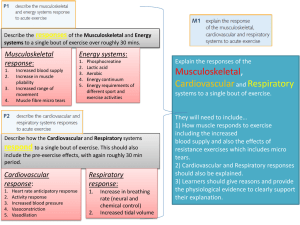
Name: DUE DATE: __________________________ Cardiovascular and Respiratory SystemsPersonal Health Evaluation Directions: You will be completing a personal health evaluation of your cardiovascular and respiratory system health. In gathering information to support your evaluation, you will need to complete the sections provided. As you complete the various sections about yourself and family members, please feel free to communicate with parent, guardian, or knowledgeable individual to gather accurate information. If you have any questions as you move through the sections, please ask! SECTION 1: Date of Birth: ______/______/_______ Height: _________ Weight: ________lbs. Sex: ____ Male ____ Female BMI Result & Category: ___________________ (BMI Categories: Underweight <18.5, Normal Weight= 18/5-24.9, Overweight 25-29.9, Obesity >30) Blood Pressure (Systolic over Diastolic) Result & Category: ____________________ (Check out this site to learn more about your risk http://www.heart.org/beatyourrisk/en_US/hbpRiskCalc.html?hasSet=true) Heart Rate: ________ (AVG Heart Rate 60-100 beats/min) Breathing Rate: _________ (AVG Breathing Rate 12-16 breaths/min) RESPONSE QUESTIONS 1. Is your BMI result of general health concern? Yes/No a. If yes, what two things can you do to reduce your BMI? If no, what two things can you do to maintain a healthy BMI? 2. Is your heart rate considered normal? Yes/No 3. Is your breathing rate considered normal? Yes/No 4. If an individual’s heart rate or breathing rate was/is significantly higher or lower than normal should he or she be concerned? Why or why not? Why might a heart rate or breathing rate indicate? 5. Why is it important to gather basic background information, such as the information above, when evaluating an individual’s potential cardiovascular and respiratory health? Be specific. Name: DUE DATE: __________________________ SECTION 2: PERSONAL MEDICAL INFORMATION: Read through the cardiovascular and respiratory system problems, check () any problems listed below that you had before or have currently. If you have/had a system problem not listed, please identify by “other.” If you have no current or history of cardio-respiratory problems, check “none.” CARDIOVASCULAR & RESPIRATORY SYSTEM PROBLEMS: High Blood Pressure/Hypertension Heart Attack Heart Failure Congenital Heart Defects (Circle CHD: ASD/VSD, Arrhythmia, Heart Murmur) Stroke Varicose Veins Anemia Hemophilia Leukemia Bronchitis Asthma Pneumonia Emphysema COPD Other: __________________________ None CURRENT SYMPTOMS: Do you have any current symptoms that may indicated a cardio-respiratory health problem? For example, coughing, wheezing, mucus, chest pain, heart palpitations, difficulty breathing, sudden weakness? Yes/No RESPONSE QUESTION 6. If yes, what symptom(s)? Will you get these examined by a medical professional? Why or why not? OR If no, why might it be wise to get such symptoms listed above examined by a medical professional right away. Give 2 reasons. SOCIAL HABITS: Check () any of your current social habits. If you check yes, please answer the follow up questions below. Do you (or have you ever used) using tobacco products? Type(s): __________________________ Frequency and Length of Use: __________________________ Do you (or have you been) exposed to second hand smoke? o Frequency and Length of Exposure: __________________________ Do you currently engage in regular physical activity? If so approximately how much per day or per week. o o o Type(s): __________________________ Frequency per Day: __________________________ Frequency per Week: __________________________ RESPONSE QUESTION Name: DUE DATE: __________________________ 7. Why do you think it’s important to look at one’s social habits when evaluating their personal health? SECTION 3: FAMILY MEDICAL INFORMATION: Complete this section about your biological family, include parents, grandparents, and sibling in your findings. If a family member has or had one of these cardiovascular/respiratory system problems please indicated their relationship to you and their name next to the specific problem. Also, be sure to include the age of onset. High Blood Pressure______________________________________ Heart Attack______________________________________ Heart Failure______________________________________ Congenital Heart Defects- ASD/VSD, Arrhythmia, Heart Murmurs______________________ Stroke______________________________________ Varicose Veins______________________________________ Anemia______________________________________ Hemophilia______________________________________ Leukemia______________________________________ Bronchitis______________________________________ Asthma______________________________________ Pneumonia______________________________________ Emphysema______________________________________ COPD______________________________________ Other (relating to CR Systems): ______________________________________ No Family Medical History of Cardio-Respiratory Problems RESPONSE QUESTION 8. Why do you think it is important for individuals to be aware of their family medical history? Name: DUE DATE: __________________________ PERSONAL CARDIO-RESPIRATORY HEALTH EVALUATION 1. What is the most important piece of information that you identified in section#1-3? Explain your reason for selection. If you didn’t collect anything of importance to you- explain how examining personal and family medical information may be beneficial for others to use. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ 2. Use the information from sections #1-3 plus what you learned about risk and protective factors, identify and explain personal risk and protective factors on the chart below. CR Factors: Gender, Ethnicity, Family History, Age, Exercise, Diet, Weight, Blood Pressure, Smoking/Smoke Exposure, and Stress. Be sure to examine all of these factors plus include any other factors that relate. RISK FACTORS PROTECTIVE FACTORS Name: DUE DATE: __________________________ 3. Using the information gathered so far, what can you conclude about your current risk for cardiovascular and/or respiratory problems? Support your response with personal evidence. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ 4. Looking at the risk and protective factors identified in question #10, go back and CIRCLE all of the Controllable Goal (I will…) Steps to Change or Maintain Resources/ Support (Set a goal regarding the factor and your (Specific action(s) your will need to take to Factor Individual (Risk or Protective) intent to maintain or change the factor) change or continue the factor) (What or who can help you reach your goal) controllable risk factors. Then select TWO of the controllable factor and rewrite the factors in the first column. Then use those factors and your knowledge of them to complete the ACTION PLAN table with detail. 5. Using the information gathered so far, plus considering that you actually apply your plan of action (created above) what can you conclude about your future risk for cardiovascular and/or respiratory diseases? Support your response with personal evidence. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Name: DUE DATE: __________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ 6. Describe your overall cardiovascular and respiratory wellness (on a scale of poor to optimal). Include information from class as well as personal and family data collection to support your response. Be as thorough as possible. Assume I know absolutely nothing about you. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Name: DUE DATE: __________________________ _____________________________________________________________________________________ _____________________________________________________________________________________