Hospital Form - 55.5 KB
advertisement

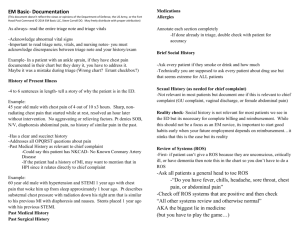
RC Health Services Emergency Medical Services Training Hospital Form – Page 1 of ____ Student Name: Date: Course Level: EMT-B EMT-I EMT-P Course Instructor: Hospital: Department: Shift: Total Hours: Preceptor Name and Certification: DSHS Number: Patient Data: Gender Male Female Age: Yr or Mo Weight: (kg) Chief Complaint/Diagnosis: MOI/NOI Complaint MOI/NOI Complaint Abdominal Pain Allergic Reaction/Anaphylaxis Animal Bite/Sting Assault/Sexual Assault Motor Vehicle Crash/Impact/Pedestrian Respiratory Difficulty/Respiratory Arrest Burns/Electrical Injury/Chemical Burn Cardiac Arrest Chest Pain/Cardiac Related Complaint Choking/Aspiration/Foreign Body Obstruction Diabetic/Endocrine Drowning/Near Drowning Fall Neurological Emergency/Seizure/CVA/TIA Possible Fracture/Dislocation/Sprain Toxic Exposure/Poisoning/Overdose Eye Injury Infection/Sepsis Pregnancy/Childbirth/Gynecological Emotional Crisis/Suicide Infectious Disease Stabbing/Cutting/Shooting Unconscious Other: Past Medical/Surgical History: Current Medications: Allergies: Glasgow Coma Scale Times Eyes Verbal Motor Pupils: Equal: Glucose: Breath Sounds Wheezes: L R Upper Lower Pain Scale Temp: Head Face Neck Chest Abdomen Pelvis Arms Legs Back/Spine Student Signature: Y Resp Vital Signs Pulse B/P Color Skin Moisture Temp. N Reactive: Y N Round: Y N Size(mm): Lt. Rt. OB/Gyn. Grav. Para. Abor. LNMP: Clear: Y N Equal: Y N Absent: L R Diminished: L R Rales: Y N Ronchi: L R Stridor: Y N Croup: Y N Upper Lower Upper Lower Upper Lower Upper Lower Onset: Severity (1-10) Quality: Radiation: SaO2: CO2: ABD Sounds: LUQ( ) RUQ( ) LLQ( )RLQ( ) Assessment Findings Assessment Findings Legend T1 abrasion M1 pain T2 amputation M2 nausea/vomiting T3 avulsion M3 abnormal sounds T4 burn M4 tenderness T5 fracture/dislocation M5 swelling T6 laceration M6 discharge T7 puncture M7 paralysis/weakness T8 bleeding, external M8 bleeding, internal T9 other trauma M9 other medical Preceptor Signature: Rev10/12 RC Health Services Emergency Medical Services Training Hospital Form – Page 2 of ____ Student Name: Date: Differential Diagnosis 1. 2. 3. Narrative Describe the appropriate pre-hospital treatment in the field for this patient (to your level of class) Briefly describe what you have learned from observing/treating this patient O – Observed Medical Abdominal CPR/Arrest ET Student Signature: A – Attempted Procedure Trauma CVA/TIA OB/Gyn Meds Patient Demographics U - Unsuccessfully P – Performed Procedure Successfully Chest Pain Diabetes EKG Allergy Syncope/AMS IV Delivery Psych Suction Respiratory Other Preceptor Signature: Rev 10/12