Session 1 09.00
advertisement

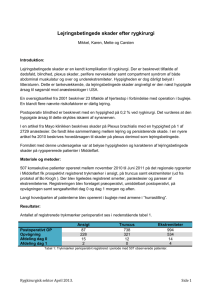
Abstracts til frie foredrag lørdag d 15/3 i forbindelse med DHS årsmøde 2014 Indholdsfortegnelse Session 1, kl. 09.00-10.20 Charlotte Madsen Christian Eskelund Ina Hahn Andreas Glenthøj Bo Mortensen Marietta Nygaard Marie Warny Mette Smith 2 3 4 5 6 7 8 9 Session 2, kl. 11.00-12.20 Michael Andersen Sarah Farmer Ulrik Ralfkjær Lasse Kristensen Simon Husby Kim Theilgaard-Mönch Andreas Ørskov Thomas Kristensen 10 11 12 13 14 15 16 17 1 Session 1 09.00-10.20 Charlotte Madsen In Transformed Indolent Lymphomas from the Rituximab Era the Efficacy of Upfront Autologous Stem Cell Transplantation Depends on When Transformation Occurs in the Course of the Disease. C. Madsen1, M. B. Pedersen1, K. Bendix2, M. B. Møller3, P. Johansen4, B. A. Jensen5, P. Jensen6, L. Munksgaard5, P. D. Brown7, E. K. Segel1, F. A. d'Amore1. 1 Department of Haematology, Aarhus University Hospital, Aarhus, Denmark, 2Department of Pathology, Aarhus University Hospital, Aarhus, Denmark, 3Department of Pathology, Odense University Hospital, Odense, Denmark, 4Department of Pathology, Aalborg University Hospital, Aalborg, Denmark, 5Department of Haematology, Odense University Hospital, Odense, Denmark, 6 Department of Haematology, Aalborg University Hospital, Aalborg, Denmark, 7Department of Haematology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark Introduction: When indolent lymphomas (IL) transform to an aggressive histology (TRIL) the result is often a rapid clinical course, treatment refractoriness and shortened survival. Although rituximab-containing chemotherapy regimens (R-chemo) has generally become standard-of-care in CD20-positive TRIL, no therapeutic gold standard has yet been established. The purpose of this study was to determine whether the outcome of TRIL patients improved if they, at the time of transformation, after R-chemo, also received upfront autologous stem-cell transplantation (ASCT). We also analyzed whether pretransformation features and prior rituximab therapy affected outcome at transformation. Patients and methods: Ninety-five patients (≤ 68 years) with histologically confirmed TRIL were included. Five-year overall (OS) and progression-free survival (PFS) were calculated and selected parameters tested in a multivariate analysis. All analyses were conducted on three cohorts: (1) whole cohort (‘all TRIL’), (2) patients with co-existing evidence of both indolent and aggressive histology at diagnosis (‘discordant/composite TRIL’) and (3) patients with indolent lymphomas transformed over time (‘sequential TRIL’). Results: Sixty-five TRIL patients (67%) received ASCT consolidation and 31 (33%) did not. Within the ‘all TRIL’ cohort, the 5-year OS and PFS for R-chemo+ASCT vs. R-chemo alone, were 65% vs. 48% (p=0.11) and 57% vs. 30% (p=0.02), respectively. At specific sub-cohort level, the ‘discordant/composite TRIL’ showed no impact of R-chemo+ASCT on neither OS (80% vs. 67%; p=0.51) nor PFS (75% vs. 61%; p=0.35). Conversely, Rchemo+ASCT improved the outcome of ‘sequential TRIL’ (OS 57% vs. 36%; p=0.09; PFS 47% vs. 6%; p=0.003), regardless of prior rituximab therapy. However, the beneficial effect of ASCT was significantly higher in patients who had not received rituximab at IL stage. Conclusions: In the rituximab era, upfront ASCT improved outcome in sequential, but not composite/discordant TRIL. Prospective trials elucidating the role of upfront ASCT in TRIL are warranted. 2 Christian Eskelund Måling af piperacillin koncentration i plasma åbner mulighed for individualiseret behandling af hæmatologiske patienter Christian Winther Eskelund1, Ingolf Mølle1, Birgitte Brock2, Tore Forsingdal Hardlei2 og Ole Halfdan Larsen1,2 Hæmatologisk Afdeling1 og Klinisk Biokemisk Afdeling2, Aarhus Universitetshospital Piperacillin med tazobactam anvendes til empirisk intravenøs behandling af neutropen feber hos patienter med maligne hæmatologiske sygdomme. Kendskabet til piperacillins farmakokinetik hos disse patienter er begrænset. Formålet med dette studie var derfor at undersøge koncentrationen af piperacillin i plasma fra hæmatologiske patienter både ved bolus dosering samt kontinuerlig behandling. Syv patienter blev fulgt med 2 daglige blodprøver under behandlingens første 5 dage. Patienterne fik initielt bolus dosering af 4g piperacillin/0,5g tazobactam intravenøst hver 8. time. Hos 6 patienter var der i observationsperioden rutinemæssigt skift til kontinuerlig infusion over 24 timer (12g/1,5g). Blodprøver blev taget gennem centralt venekateter. Piperacillin koncentrationen blev kvantificeret ved en UHPLC metode (Agilent 1290). De inkludererede patienter var alle mænd med maligne hæmatologiske sygdomme og neutropeni på grund af kemoterapi. Ved behandlingsstart var temperaturen 38.4°C (38.2-38.7) (median (interkvartil interval)) og TOKS score 3 (1-4). Der blev observeret markante interindividuelle forskelle i median piperacillin peakværdi: 171 µg/mL (107-190), halveringstid: 35 min (29-42) samt niveau ved steady state under kontinuerlig behandling: 18 µg/mL (13-21). Der var ikke tegn til signifikant ændring over tid (ANOVA p-værdier > 0.34). Interindividuelle forskelle kunne kun delvis forklares ved forskelle i kropsvægt (R2 0.18-0.30). Nyrefunktionen var normal hos de undersøgte og bidrog ikke til de observerede forskelle (alle R2<0.18). Dette studie viser at måling af piperacillin kan anvendes til monitorering af behandlingen hos hæmatologiske patienter. Den nye metode påpeger markante interindividuelle forskelle og åbner mulighed for individualiseret behandling med optimeret effekt og bivirkningsprofil. Den fulde potentielle kliniske værdi heraf bør afklares i et større klinisk randomiseret studie. 3 Ina Hahn Prevalence of venous thromboembolism in patients with Diffuse large B-cell lymphoma Ina Hornemann Hahn1; Jakob Madsen1; Marianne Tang Severinsen1 1Department of Haematology, Aalborg University Hospital, Aalborg Introduction: Venous thromboembolism (VTE) is a critical complication in patients with cancer but the information on VTE among patients with diffuse large B-cell lymphoma(DLBCL) is sparse. We aimed to evaluate the incidence of VTE in patients with DLBCL and to evaluate the quality of registry data on VTE among DLBCL patients. Methods: Patients with a first time diagnose of DLBCL at the Department of Haematology Aalborg University Hospital from January 1, 2007 to December 31, 2013 were included in the study. Participants were followed from date of DLBCL and two years further. We reviewed the entire medical records for all DLBCL patients and data on confirmed VTE events were retracted. Also VTE risk factors, medication, platelet count, haemoglobin and leukocyte count at date of VTE were noted. We retracted register data on VTE discharge diagnosis from Patients Administrative System from the participants and compared this with information from medical records on VTE events. Results: A total of 296 patients had an incident diagnosis of DLBCL during the study period. We identified 32 (10.8%) with a VTE event within a two-year follow-up period of which three PEs were found on routine CT scan. In the discharge register 20 of the 296 patients had a diagnosis of VTE during follow-up of which 17 were confirmed. The positive predictive value of a VTE discharge diagnosis was 85%. Only 17 of the 32 confirmed VTE cases were registered therefore the sensitivity of a VTE discharge diagnosis was 53%. Conclusions: 10,8 % DLBCL patients had a VTE event during two years of follow-up. Register data on VTE discharge diagnosis is valid among patients with DLBCL with a positive predictive value of 85%. The sensitivity of a VTE discharge diagnosis among DLCBL patients is only 53%. 4 Andreas Glenthøj PLASMA PROHNPS ARE SPECIFIC EARLY MARKERS OF NEUTROPHIL ENGRAFTMENT IN PATIENTS UNDERGOING HIGH-DOSE CHEMOTHERAPY, AUTOLOGOUS OR ALLOGENEIC STEM CELL TRANSPLANTATION Andreas Glenthøj, Frederik Emmertsen, Jette Sønderskov, Peter Kampmann, Henrik Sengeløv, Niels Borregaard. Department of Hematology, Rigshospitalet, Copenhagen, Denmark 1.0 2.5 0.8 2.0 0.6 1.5 0.4 1.0 0.2 0.5 0.0 PMN proHNPs PMNs 109/L Relative to max Background: Neutropenia is invariably a consequence of myeloablative conditioning before hematopoietic stem cell transplantation (SCT) as well as high-dose chemotherapy. Several plasma proteins have been investigated as early markers of bone marrow recovery, but these lack specificity which renders them clinically less useful. Human neutrophil peptides (HNPs) are antimicrobial peptides exclusively synthesized by neutrophil precursors. Most is synthesized by myelocytes, where HNPs remain unprocessed as proHNPs and are secreted in large amounts to the bone marrow plasma, and from here to blood. Aims: We hypothesized that proHNPs may serve as early and specific markers of granulopoiesis in patients undergoing hematopoietic SCT or high-dose chemotherapy. Methods: Plasma samples were obtained daily from patients undergoing allogeneic SCT (n=11), autologous SCT (n=16), or high-dose chemotherapy (n=14). Furthermore, plasma samples were taken from patients with AML prior to chemotherapy (n=19) and healthy controls (n=39). ProHNPs, MPO, NGAL, and lysozyme were measured by ELISA. Results: Neutrophils disappeared rapidly from circulation after myeloablative conditioning or highdose chemotherapy. Of the investigated proteins, only proHNPs consistently disappeared from circulation along with neutrophils. Likewise, only proHNPs invariably preceded the rise in neutrophils. In patients undergoing allogeneic SCT, proHNPs rose five to six days before neutrophil counts. Patients undergoing autologous SCT were treated with G-CSF to speed up neutrophil recovery and in these, proHNPs rose approximately two days before neutrophils were detected. As for patients receiving induction or consolidation chemotherapy, proHNPs predated neutrophils by two to four days. Patients with AML had significantly lower levels of plasma proHNPs than healthy controls, indicating that proHNPs are not produced by leukemic blasts. Conclusion: ProHNPs are markers of normal granulopoiesis. Clinically, plasma proHNP could be an important tool to distinguish late take from primary graft failure in hematopoietic SCT patients, since measurement of proHNPs in plasma allows early detection of donor cell engraftment. 0.0 0 5 10 15 20 25 Day Figure 1: ProHNPs and polymorphonuclear neutrophils (PMNs) in peripheral blood of one patient undergoing allogeneic SCT. Patient is representative of the group. Day 0 marks the day of SCT. 5 Bo Mortensen Similar long term overall survival after allogeneic HCT for severe aplastic anemia in patients transplanted with a related donor compared to an unrelated donor Mortensen BK, Jacobsen N, Heilmann C, Sengeløv H. Department of Hematology, National University Hospital, Rigshospitalet, Copenhagen, Denmark Treatment of severe aplastic anemia (SAA) is based on immunosuppressive therapy (IST) and allogeneic hematopoietic cell transplantation (HCT). For patients younger than 55 years with an HLA-identical sibling donor, allogeneic HCT is the treatment of choice. For patients younger than 55 years who lack an HLA-identical sibling donor, IST is the treatment of choice and allogeneic HCT is recommended after failure to respond to IST. We retrospectively analysed the outcome of all patients treated with allogeneic HCT for SAA at Rigshospitalet between 1977 and 2013 and compared the outcome of allogeneic HCT for patients transplanted with a related donor vs. an unrelated donor. The median age at HCT was 16 years (0-61). The donor was an HLA-identical sibling in 51 (53 %), syngen in 2 (2 %), related HLA mismatched in 4 (4 %), HLA matched unrelated in 29 (30 %), and HLA mismatched unrelated in 10 (11 %). Forty-five (47 %) patients were transplanted between year 1977 and 2000, and 51 (53 %) were transplanted after year 2000. Overall survival (OS) in patients transplanted before 2000 was 58 %, whereas survival after 2000 increased to 92% (P<0.0001), median observation times were 15,0 years (0-33) and 5,4 years (0-13), respectively. In patients transplanted after year 2000, OS was 89% both after transplantation with a related donor or an unrelated donor (figure 1) (Fig 1). Median observation times were 6,5 years (0-13) and 4,1 years (0-11), respectively. In this study we observe a marked improvement in survival among SAA patients receiving an allogeneic HCT since 2000. Interestingly, we find similar long term OS in patients transplanted with a related donor as compared to an unrelated donor. Our study supports, that allogeneic HCT with an unrelated donor should be considered as first line treatment in selected patients with SAA lacking an HLA-identical sibling donor. Figure 1: Overall survival in patients transplanted for SAA after year 2000 with a related or an unrelated donor: 6 Marietta Nygaard Close Monitoring of Cyclosporine A Concentration as a Means of Preventing Acute Graft-versus-Host Disease in Allogeneic Stem Cell Recipients Nygaard M, Hovgaard D, Schjødt I, Smedegaard Andersen N, Vindeløv L and Sengeløv H Department of Hematology, Rigshospitalet, Copenhagen University, Copenhagen, Denmark Introduction The whole blood concentration of cyclosporine A (CsA) after allogeneic stem cell transplantation is important in prevention of acute graft versus host disease (aGVHD). Low concentrations may cause aGVHD and high concentrations toxicity or relapse. The target concentration and method of monitoring and administering CsA varies between transplant centers. As one of few centers we measure CsA daily and furthermore administer CsA orally for as long as possible. Methods We retrospectively analyzed data from 48 adult patients, who consecutively underwent myeloablative allogeneic stem cell transplantation in the years 2010 and 2011 at Rigshospitalet. Transplant indications were AML (n=18), ALL (n=14), MDS (n=3), SAA (n=6), MM (n=2) and other (n=5). Whole blood concentration of CsA was measured once daily. The median CsA concentration in weeks 1 to 4 was calculated, and patients were divided into two equally sized groups according to the median CsA concentration. Renal impairment was defined as doubling of serum creatinine during the first 28 days after transplantation. Results Assessing the cumulative incidence of aGVHD with death as competing event, the proportion of patients with aGVHD grade II-IV was higher in those with CsA levels below the median in week 2 after transplantation (p=0.012, figure 1). CsA levels were not correlated with excess risk of renal impairment or death from relapse. 21 patients (43%) received CsA orally for the entire transplantation period. There was no difference in occurrence of aGVHD between groups on intravenous and oral CsA (p=0,2). Conclusion Close monitoring of the CsA concentration in the early transplant period is important in maintaining CsA within target concentration and thus preventing aGVHD. Target concentration of CsA should possibly be adjusted to higher levels than we observed in this series of patients. It seems safe to administer CsA orally with regards to aGHVD. Figure 1 Cumulative incidence of aGVHD (1) and death (2) for groups with high and low CsA. 7 Marie Warny G6PD deficiency in the Danish immigrant population Marie Warny, Jesper Petersen, Tobias Wirenfeldt Clausen and Henrik Birgens Hæmatologisk afdeling, Herlev Hospital Abstract Glucose-6-phosphate dehydrogenase (G6PD) deficiency is a common occurring enzyme deficiency, with a high prevalence in areas historically exposed to malaria. In this study 1508 Danish immigrants (307 males and 1201 females) were tested using quantitative and molecular methods, to determine the prevalence of G6PD deficiency in the Danish immigrant population. We found the allelic frequency to be 2,7% in the female population. Furthermore, a map of the mutation pattern in the Danish immigrant population was made, 202A showing a high prevalence of the G6PD Avariant in African immigrants, a high prevalence of the G6PD Mediterranean variant in immigrants coming from the Mediterranean and western Asia countries and a high variant heterogeneity in the populations of the South East Asia-Pacific. The Danish immigrant population from the abovementioned areas, is characterized by a high prevalence of thalassaemia trait, and thus microcytosis and low mean corpuscular haemoglobin (MCH). The lowered mean haemoglobin content of the red blood cells, cause deviations in the G6PD activity when measured as activity per g of Hgb. Since this study included many patients with various thalassemic syndromes it gave us an opportunity to evaluate the interaction between a thalassemia gene and the G6PD gene on the clinical phenotype especially in heterozygous females. We found some overlap between patients without G6PD deficiency and heterozygous females, but the positive predictive value of a sample with low or intermediate activity of G6PD was highly influenced by the MCH level. Measuring MCH is a helpful tool to evaluate whether a female with seemingly normal G6PD activity is at risk of being heterozygous G6PD deficient or not. Figure: It is obvious that there is no diagnostic trouble concerning males, since their G6PD activities is split in two, those with normal activity and those with abnormal activity. Three G6PD hemizygous males with near-normal activity (Δ), all had blood transfusion prior to the quantitative assay. Females are more difficult to classify, in that there is no clear distinction between the three activity levels. This is consistent with the problem in diagnosing heterozygous females, because they present a broad spectrum of activities. 8 Mette Smith Red cell mass measurement in the diagnostic of PV and ET anno 2013 Mette Aaby Smith(1), Anders Møjbæk(1), Allan Johansen(2), Hanne Vestergaard(3) 1: stud med, SDU, 2: ledende overlæge, Nuklearmedicinsk afdeling, OUH, 3: konst. ledende overlæge, PhD, Hæmatologisk afdeling, OUH Introduction and background: Essential thrombocytosis (ET) and polycythemia vera (PV) belong to the Philadelphia chromosome-negative chronic myeloproliferative neoplasms (MPN). After the discovery of the JAK2 mutation, WHO in 2008 changed the diagnostic criteria for PV and ET, omitting the measurement of red cell mass (RCM) and replacing it with haemoglobin measurements. Patients with early PV may be difficult to discriminate from patients with ET. The aim of this study was to clarify to what extent EV determination contributes to the differential diagnosis between PV and ET and to the diagnosis of PV. Methods and results: From 2007 to 2012, a total of 95 patients were referred from the Department of Haematology X, Odense University Hospital, for RCM measurement. Of these, 79 patients were included in the study and assigned to one of two groups, depending on whether they presented with thrombocytosis (study population) or with a normal number of thrombocytes (the rest). In the study population, 21 patients had normal haemoglobin and haematocrit values. Twelve of these had increased RCM, and they were diagnosed with PV. Nine of these patients did not get their final diagnosis till after the RCM measurement. Conclusion: RCM measurement contributes to the differential diagnosis between PV and ET, and it is necessary to include it for patients presenting with isolated thrombocytosis. 9 Session 2 11.00-12.20 Michael Andersen Korrelation mellem hypogammaglobulinæmi og cytogenetiske aberrationer og paraklinisk karakteristik af en CLL kohorte fra en enkelt institution. Michael A Andersen, Ole W Bjerrum, Mette Klarskov Andersen og Christian Geisler Hæmatologisk Klinik, Rigshospitalet Karakterisering af hypogammaglobulinæmi, cytogenetiske aberrationer og IGVH mutationsstatus kan hjælpe til forståelse af patogenese, sygdomsprogression og immundefekt for B-CLL. Forekomsten af lave immunglobulinniveauer er ikke undersøgt i forhold til de cytogenetiske abnormiteter. Det primære formål med studiet var at undersøge sammenhænge mellem Ig A, G og M, IGVH og cytogenetiske aberrationer. Det sekundære formål var at korrelere parametre i nyligt diagnosticerede CLL-patienter for at illustrere sammenhænge i sygdomsbiologi. Metode Journalen fra 97 konsekutive patienter over 3 år, identificeret ved DRG kode, blev gennemgået for at registrere de kliniske, patologiske og cytogenetiske karakteristika retrospektivt. Resultater En reduktion i mindst en af immunglobulinklasserne blev observeret i 57 %. IgA var lavt hos 23 % af patienterne, 17 % havde lavt IgG og 52 % af patienterne havde lavt IgM niveau. Blandt de 75 % af patienterne med mindst en anomali havde 48 % 13q deletion, 17 % havde trisomi 12, 7,7 % havde 17p deletion, 6,6 % havde 11 q deletion og 6,6 % havde 14q32 translokation. Patienter med trisomi 12 viste signifikant forhøjet IgA- og IgG-niveau. Patienter med 14q32 translokationer havde signifikant lavere IgA og IgG. Statistisk signifikante korrelationer blev demonstreret mellem stadier og rutine parakliniske parametre. Konklusioner 1. Ved trisomi 12 var IgM og IgA signifikant forhøjet. Patienter med 14q32 translokation havde signifikant nedsat IgA og IgG. Det indikerer, at genetiske forhold på kromosom henholdsvist 12 og 14 kan have betydning for regulering af immunglobulin. 14q32 translokation involverer IGH genet, hvilket kan have betydning herfor. 2. Statistisk signifikante sammenhænge kunne demonstreres for en række rutine blodprøver, hvilket illustrerer CLLs biologi. Princippet kan bruges som en indikator for at dokumentere anvendelse af en repræsentativ CLL population i behandlings- eller studie sammenhæng. 10 Sarah Farmer Bone manifestations in patients with myelofibrosis - A cross-sectional study using DXA and HR-pQCT. Sarah Farmer1, Pernille Hermann2, Vikram Shanbhogue2, Stinus Hansen2, Hanne Vestergaard1, Claudia I Stahlberg3, Henrik Frederiksen1 1 Department of Hematology, 2Department of Endocrinology, 3Department of Pathology, Odense University Hospital, Odense, Denmark Objectives In patients with myelofibrosis, osteosclerotic changes appear in the bone tissue as the result of growing and thickening of the bone trabeculae. We conducted a cross-sectional study to evaluate bone structure MF patients using conventional DXA and High-resolution peripheral quantitative CT (HR-pQCT). Materials and Methods Patients who meet the diagnostic criteria of primary myelofibrosis or myelofibrosis secondary to another CMPN according to WHO 2010-criteria with International Classification of Diseases, 10th revision, from the department of haematology, Odense University Hospital, Denmark were included. Areal Bone mineral density was assessed by DXA (duel energy X-ray absorption), and 3D assessment of Bone geometry, volumetric BMD, and micro-architecture were measured using HRpQCT Data are compared with healthy volunteers matched on age, sex, and height, in a 1:1 ratio. Blood samples were analyzes for PINP1 (procollagen type I N-terminal pro-peptide), a markers of bone formation. Diagnostic bone marrow biopsies were reviewed by a hematopathologist to confirm diagnosis, classification of fibrosis grade and presence of osteosclerotic changes. Results 20 MF patients were included, 11 with grade 1-2 and 9 with grade 3. Mean age was 69.8 (95% CI: 66.3-73.4). BMD in patients were increased in spine 1.10 (0.93-1.08) vs. 0.93 (0.87-1.00), but not of the hip 0.93 (0.85-1.02) vs. 0.90 (0.82-0.98) and HR-pQCT showed increased bone mass, particular trabecular volumetric BMD, trabecular BV/TV, and trabecular number, although statistical significance was not reached. PINP was increased in patients (fig 1). Conclusion This study demonstrated elevated level of PINP in MF patients indicating increased formation rate of collagen 1 correlated to new bone formation. DXA indicated increased bone mass, and the HRpQCT could locate this predominately on trabecular site. Myelofibrosis is a rare disease and the number of patients included was small. MF patients 50 100 150 Healthy donors 0 Ulrik Ralfkjær Level of PINP (ng/mL) 11 Ulrik Ralfkjær The role of microRNA 203 in cutaneous T-cell lymphoma [1,2] [2] [3] [4] [5] [5] Ralfkiær U, Kopp KL, Gjerdrum LM, Marstrand T, Ahler CB, Glue C, [4] [6] [7] [3] [2] [2] Røpke M, Gniadecki R, Skov L, Ralfkiær E, Woetman, A, Ødum N and [1] Grønbæk K [1] [2] Rigshospitalet, dept. of Hematology, University of Copenhagen, dept. of International Health, [3] [4] [5] Immunology and Microbiology, Rigshospitalet, dept. of Pathology, LEO Pharma, Exiqon, [6] [7] Bispebjerg Hospital, dept. of Dermatology and Gentofte Hospital, dept. of DermatoAllergology Cutaneous T-cell lymphoma (CTCL) is a rare disease which originates from malignant transformation of skin homing memory T-cells. A major challenge in CTCL is early diagnosis, since the early phases often resemble benign skin disorders (BSD) both clinically and histologically. As a result many patients are followed for years with repeated examinations by morphology, pheno-typing and geno-typing before a definite diagnosis and relevant therapy can be initiated. MicroRNAs (miRs) constitute a novel class of noncoding RNA that are expressed in a cell and tissue specific manner in both normal and malignant tissues. In this study we have focused on miR expression in CTCL vs. benign diseases. The first aim of this project has been to develop a diagnostic kit, which can assist in establishing an early diagnosis. We used Exiqon miR microarrays to show that the expression level of 3 miRs (203, 205 and 155) can discriminate CTCL from BSD with >95% classification accuracy (Ralfkiaer U, Hagedorn PH et al., Blood. 2011 Nov 24). We validated these findings in an independent cohort using a TaqMan qPCR based method Marstrand et al., Leuk Lymphoma. 2013 Jul 29). The second aim of this project has been to investigate the regulation and function of miR203 in CTCL. MiR-203 is critical for normal development of stratified epithelia and acts to repress stemness and induce differentiation. Consistent with this function in normal cells, miR-203 is down-regulated in many cancers and has been recognized as an important tumor suppressor in both epithelial and hematological malignancies. We show that miR203 is down-regulated in CTCL compared to BSD and normal blood T-cells, and that a probable cause of this down-regulation is epigenetic silencing by DNA promoter methylation. We also show that induced miR-203 expression in transfected cells targets known the oncogenes, p63, survivin and cREB. To search for new potential targets of miR203, miR-203 mimic and mock transfected cells were examined on Affymetrix gene expression arrays. This resulted in the identification of a list of 19 significantly de-regulated genes, including a previously unrecognized miR-203 target molecule involved in cytokine induced JAK/STAT signaling, a pathways frequently aberrantly activated in CTCL. In conclusion, we have identified a miR classifier that may aid early recognition of CTCL and have added significant novel insight into the possible biological means of action of mir203 in CTCL pathogenesis. 12 Lasse Christensen Investigation of allelic methylation patterns of the death-associated protein kinase (DAPK) gene in diffuse large B-cell lymphoma (DLBCL) using a novel pyrosequencing-based method. Lasse Sommer Kristensen1, Marianne Bach Treppendahl1, Fazila Asmar1, Mia Seremet Girkov1, Helene Myrtue Nielsen1,2, Tina Ellegaard Kjeldsen2, Elisabeth Ralfkiaer3, Lise Lotte Hansen2 & Kirsten Grønbæk1 1 Department of Hematology, Rigshospitalet, Copenhagen, Denmark. Department of Biomedicine, Aarhus University, Aarhus, Denmark. 3 Department of Pathology, Rigshospitalet, Copenhagen, Denmark. 2 Background: Diffuse large B-cell lymphoma (DLBCL) is the most common type of nonHodgkin’s lymphoma in the western world. Improvements in overall survival have been observed with the introduction of rituximab in combination with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), however, prognostic markers are still needed. Methylation of the death-associated protein kinase (DAPK or DAPK1) gene is likely to have prognostic value in DLBCL patients treated with R-CHOP. Findings: Allele-specific methylation patterns of the DAPK promoter CpG island were assessed using allelic MSP-pyrosequencing in a cohort of 106 DLBCL patients uniformly treated with R-CHOP. Mutation status of the TP53 gene was assessed using denaturing gradient gel electrophoresis (DGGE) and Sanger sequencing for 80 of the patients. DAPK mono- and biallelic methylation was associated with shorter overall survival (p =0.029). When only considering individuals heterozygous for the rs13300553 SNP a shorter overall survival was associated with monoallelic methylation of the A-allele (p =0.005). Patients carrying both DAPK methylation and a TP53 mutation did not have a statistically significant difference in overall survival compared to patients carrying only one of these molecular alterations (p =0.134). Conclusions: This study confirms the potential of DAPK methylation as a prognostic marker in DLBCL. Moreover, monoallelic methylation of the A-allele of the rs13300553 DAPK promoter CpG island SNP is associated with inferior overall survival as compared to all other allelic DAPK methylation patterns. 13 Simon Husby miRNA-18b overexpression identifies mantle cell lymphoma sub-group with poor survival and improves MIPI-B prognostication Simon Husby1*, Ulrik Ralfkiaer1*, Christian Garde2,9, Sara Ek5, Arne Kolstad3, Mats Jerkeman4, Anna Laurell5, Riikka Räty6, Mats Ehinger5, Christer Sundström7, Marja-Liisa KarjalainenLindsberg6, Jan Delabie3, Elisabeth Ralfkiaer8, Erik Clasen-Linde8, Peter Brown1, Christopher T. Workman2,9, Christian H. Geisler1# and Kirsten Grønbæk1#. Purpose Mantle cell lymphoma (MCL) is an aggressive rare NHL subtype with a variable clinical course. We assessed whether MCL miRNA expression could identify patients with poor survival and improve current prognostication of MCL patients. Patients and Methods Diagnostic MCL samples from 172 patients in the Nordic MCL2 and MCL3 clinical trials were retrieved. All patients had confirmed CyclinD1 overexpression and received high dose immunochemotherapy followed by ASCT. The median follow-up was 6.4 years for the MCL2 cohort and 3.7 years for the MCL3 cohort. Genome-wide miRNA microarray profiling was performed in 74 patients of the screening cohort (MCL2). Differentially expressed miRNAs (adjusted p-value < 0.05) were re-analyzed by qRT-PCR. Prognostic miRNAs were validated by qRT-PCR in 94 patients of the validation cohort (MCL3). Results In the screening cohort 17 miRNAs were differentially expressed by microarray analysis in patients who died from MCL. Follow-up qRT-PCR analysis found that 3 of the 17 miRNAs (miR18b, miR-92a, miR378d) were differentially expressed in patients who died from MCL in the validation cohort. On the basis of data from the screening cohort, feature selection and leave-oneout cross-validation, miR-18b was identified to hold the highest prognostic value. We generated a new MIPI-B-miR prognosticator, by combining expression-levels of miR-18b with MIPI-B data, which improved prognostication compared to the current gold standard with regards to causespecific survival, overall survival and progression-free survival. Conclusion Overexpression of miR-18b identifies patients with poor prognosis in two large prospective MCL cohorts and adds prognostic information to the MIPI-B prognosticator. 14 Kim Theilgaard-Mönch Comparing cancer vs. normal gene expression profiles identifies common transcriptional cancer programs in AML patients. Nicolas Rapin1,2,3,4, Frederik Otzen Bagger1,2,3,4, Johan Jendholm1,2,4, Helena MoraJensen5, Anders Krogh2,3, Alexander Kohlmann6, Christian Thiede7, Niels Borregaard5, Lars Bullinger8, Ole Winther2,3,9, Bo T. Porse1,2,4,11, Kim Theilgaard-Mönch1,2,10,11 1 The Finsen Laboratory, Rigshospitalet, Faculty of Health Sciences, University of Copenhagen, Denmark; 2Biotech Research and Innovation Centre (BRIC), University of Copenhagen, Copenhagen, Denmark; 3The Bioinformatics Centre, Department of Biology, Faculty of Natural Sciences, University of Copenhagen; 4Danish Stem Cell Centre (DanStem) Faculty of Health Sciences, University of Copenhagen, Denmark; 5The Granulocyte Research Laboratory, Rigshospitalet, Faculty of Health Sciences, University of Copenhagen, Denmark; 6MLL Munich Leukemia Laboratory, Munich, Germany; 7University Hospital Carl Gustav Carus, Medical Dept. 1, University of Technics Dresden, Germany; 8Department of Internal Medicine III, University Hospital of Ulm, Ulm, Germany; 9DTU Compute, Technical University of Denmark, Lyngby, Denmark: and 10 Dept. of Hematology, Skanes University Hospital, University of Lund, Sweden, 11These authors contributed equally to this work Gene expression profiling (GEP) has been used extensively to characterize cancer, identify novel cancer entities and improve patient prognostification. However, it has largely failed to identify transcriptional programs that differ between cancer and corresponding normal cells, and are fundamental to disease etiology. Here we report a newly developed method that facilitates the comparison of any cancer sample to its nearest normal cellular counterpart and apply this method using acute myeloid leukemia (AML) as a model. First we generated a gene expression-based landscape of the normal hematopoietic hierarchy using expression profiles from highly purified normal hematopoietic stem/progenitor cells (HSPCs) and their mature myeloid progeny, and mapped gene expression profiles of AML patients to this landscape. This allowed us to identify the closest normal cell population for individual AML samples and determine gene expression changes between cancer and normal. We find the cancer vs. normal method (CvN-method) to be superior to conventional methods in stratifying AML patients with aberrant-karyotype (AK-AML). Moreover, the CvN-method uncovered a novel poor-outcome subtype of normal-karyotype AML (NK-AML), which allowed for the generation of a highly prognostic survival signature. Our analysis also unraveled common transcriptional programs that are associated with elevated signaling activity, inflammatory response and hypoxia. Strikingly, these common transcriptional programs are shared by most AML patients despite their otherwise profound clinical and genetic heterogeneity. As these common transcriptional programs represent disrupted core cellular functions including aberrant oncogenic pathway activity some of them are highly relevant for targeting by antibody- and small molecule-based therapies. Collectively, our study implicates that our CvN-method holds great potential as a tool for prognostification as well as the identification of transcriptional cancer programs for future targeted therapies. 15 Andreas Ørskov Is there a rationale for combined targeting of PD-1 and DNA methylation in myelodysplastic syndrome? Ørskov AD, Treppendahl MB and Grønbæk K Epi-/Genome Laboratory, Dept. of Hematology, Rigshospitalet, Copenhagen Introduction: The programmed death-1 (PD-1) is a molecule that is involved in immunosuppression. It is expressed on activated T-cells and inhibits T-cell function upon binding to its ligand B7-H1. Numerous cancer studies indicate that the tumour microenvironment manipulates the PD-1/B7-H1 pathway by upregulating B7-H1 on tumour cells. The demethylating agent, azacytidine (AZA), is used as standard therapy for higher risk MDS patients; however, the majority of the patients will lose their response to AZA over time. It has recently been shown that the expression of PD-1 is regulated by DNA methylation. Accordingly, we suggest that AZA, in addition to its beneficial function, induces the PD-1 expression on T-cells in the MDS microenvironment thereby hampering the immune response against the MDS blasts. + + Methods: CD4 and CD8 T-cells from MDS patients sampled before and during AZA treatment were isolated by magnetic cell sorting. PD-1 promoter methylation was analysed by pyrosequencing. PD-1 expression was analysed by RT-qPCR and cell surface expression will be analysed by flowcytometry. The expression of B7-H1 on MDS blasts from the same patients will be analysed by flowcytometry. Results: 20 MDS patients have currently been analysed. Our preliminary results demonstrate an ongoing demethylation of the PD-1 promoter in the T-cells during treatment with AZA in ~60% of the patients. The demethylation is accompanied by an upregulation of the PD-1 mRNA expression. Data on cell surface expression of PD-1 and B7-H1 will be presented at the meeting. Discussion: The first and very preliminary results of this study suggest that PD-1 signalling may be involved in MDS pathogenesis and in resistance to AZA. Based on these preliminary data we hypothesize that the combination of AZA and PD-1/B7-H1 pathway inhibitors may be efficient therapy in AZA refractory MDS. 16 Thomas Kristensen Clinical relevance of sensitive and quantitative STAT3 mutation analysis using next generation sequencing in T-cell large granular lymphocytic leukemia Thomas Kristensen1, Martin Larsen2,3, Annika Rewes4, Henrik Frederiksen4. Mads Thomassen2,3, Michael Boe Møller1 1 Department of Pathology, Odense University Hospital, 2Department of Clinical Genetics, Odense University Hospital, 3Human Genetics, Clinical Institute, University of Southern Denmark, 4 Department of Hematology, Odense University Hospital, Odense, Denmark Abstract: Diagnosis of T-cell large granular lymphocytic leukemia (T-LGL) is often challenging because clinical and laboratory characteristics are overlapping with nonneoplastic conditions. Recently, mutation in the STAT3 gene has been identified as a recurrent genetic abnormality in T-LGL. STAT3 mutation therefore represents a promising marker in T-LGL diagnostics. We therefore developed a new quantitative next generation sequencing (NGS) assay that allows sensitive analysis of the STAT3 gene. The assay was used to study the utility of STAT3 mutation analysis as a diagnostic tool in T-LGL. Sixteen T-LGL patients were included in the study. A total of 15 mutations, including two new mutations (G618R and K658R), were detected in 12 patients (75%) with mutation levels ranging from 2.5 – 45.6% mutation positive alleles. NGS detected 50% more mutations than Sanger sequencing. Blood samples from 20 healthy blood donors all tested negative, thus demonstrating the specificity of the assay. Also, the results indicated that mutation levels in blood and bone marrow are not systematically different and that NGS-based STAT3 mutation analysis represents a sensitive method for monitoring of residual disease as demonstrated in a patient receiving pentostatin. In conclusion, we demonstrate the clinical relevance of NGS-based STAT3 mutation analysis which represents a sensitive and specific diagnostic marker in T-LGL that allows assessment of molecular residual disease which may improve clinical decision making. 17 A common Nordic/Baltic treatment strategy for children and adults (1- 45 years) with acute lymphoblastic leukaemia Kjeld Schmiegelow, Department of Paediatrics & Adolescent Medicine, Rigshospitalet Copenhagen, kschmiegelow@rh.dk Historically, adolescents and adults with acute lymphoblastic leukaemia have had a significantly poor cure rate than young children with ALL. For both children and adults treatment has primarily been based on clinical characteristics at diagnosis (age, tumour burden, immune phenotype, cytogenetics) and time to obtained morphological remission. With intensive chemotherapy, prophylactic and therapeutic cranial irradiation for high-risk patients, and haematopoietic stem cell transplantation for the highest risk group, the eventfree survival obtained has been 80 % for children and approximately 40 % for patients 1845 years of age. Since July 2008 a common treatment protocol has been used for all children with ALL (1-18 years) in Denmark, Norway, Sweden, Iceland, Finland, Estonia, and Lithuania, and an increasing number of adult departments of hematology have joined this strategy, which now includes all adults of 18-45 years in Denmark, Norway, Sweden, Estonia, Lithuania, and Helsinki. Risk grouping (i.e. treatment intensity) is based on cytogenetics and minimal residual disease in bone marrow after one and three months of therapy. No patients receive cranial irradiation during first remission, and transplantation is only offered to patients not being in remission at the end of induction therapy or who has a tumour burden above 0,1 % in bone marrow after three months of therapy. With more than 1300 patients included (>200 above 18 years), the five year event-free survival for children (1-18 years) is now 85 % and the event-free survival for adults is identical to that of children, if survival analyses are stratified by risk group. Thus, the overall event-free survival for adults is only slightly lower than that for children due to a higher frequency of T-cell ALL, MLL rearrangements, and poorer MRD-response at end of induction therapy. In addition to significant improvements in cure rates, the common Nordic/Baltic treatment strategy is a unique platform for future research. 18

![[Session A] Kontakten til sundhedsvæsenet](http://s3.studylib.net/store/data/009732071_1-90e7c7dc246805d636794996a581b450-300x300.png)