Informed Consent For Therapy Services
advertisement

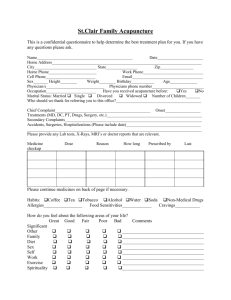
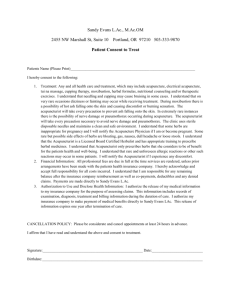
Informed Consent for Therapy Services Welcome to our Center and thank you for allowing me to help you on your path toward health and wellness. This document contains important information about my professional services and our Center’s business policies. Please read it carefully and jot down any questions you might have so that we can discuss them at our next meeting. When you sign this document, it will represent an extension of the initial, verbal agreement between us. Acupuncture Treatment and Care I understand that methods or treatment may include, but are not limited to, acupuncture, acupressure, press pellets, electrical stimulation, Chinese or Western herbal medicine and nutritional or lifestyle counseling. I have had the opportunity to discuss with the acupuncturist named below and/or with other office or clinic personnel the nature and purpose of acupuncture treatments and other procedures. Acupuncture attempts to normalize physiological functions, to modify the perception of pain, and to treat certain diseases of dysfunctions of the body. I have been informed that acupuncture is a safe method of treatment, but occasionally there may be some bruising or tingling near the needling sites that last a few days. There have been very rare instances reported of fainting, infection and scarring. There have been extremely rare instances reported of needle breakage, spontaneous miscarriage and pneumothorax. There may be some bruising after cupping. The herbs and nutritional supplements (which are from plant, animal and mineral sources) that have been recommended are traditionally considered safe in the practice of Chinese Medicine. I understand that some herbs may be inappropriate during pregnancy. If I experience any gastrointestinal upset or allergic reactions to the herbs, I will inform the acupuncturist. I do not expect the acupuncturist to be able to anticipate and explain all risks and complications. I wish to rely on the acupuncturist to exercise judgment during the course of the procedure, which the acupuncturist feels at the time, based upon the facts then known, is in my best interests. I understand the clinical and administrative staff may review my medical records and lab reports, but all my records will be kept confidential and will not be released without my written consent. I have read, or have had read to me, the above consent. I have also had an opportunity to ask questions about its content. BILLING AND PAYMENT Unless otherwise agreed, the hourly fee for acupuncture at the Claret Center is $80.00. You will be expected to pay for each session at the time it is held, unless we agree otherwise. We will provide an electronic receipt of treatment that you can use to submit to your Insurance Company. We are not responsible for acceptance/rejection by your Insurance Company. Under certain circumstances, fee adjustments or installment plans may be negotiated. 5536 S. Everett Avenue Chicago, IL 60637 Phone (773) 643-6259 www.claretcenter.org Informed Consent for Therapy Services This form acknowledges that you have requested professional services from me and have received a copy of the Claret Center Informed Consent for Services. This letter sets forth the agreement concerning our understanding of such services. 1. You are entitled to receive information from me about my methods, techniques, education and credentials. You have the right to stop talking to me at any time, and/or to seek a second opinion about your concerns. 2. We both understand that it is never permissible for a sexual relationship to develop between a client and a therapist. 3. Our conversations are confidential. I will not share anything we discuss with anyone else unless I get your written permission. 4. If you participate in whatever services are recommended by me, you agree to pay for these professional services according to the fee schedule you have received. 5. You will be charged for missed appointments cancelled less than 24 hours in advance. 6. Returned Checks: A service charge will be applied for checks returned by your bank for any reason. If two or more checks are returned, Claret Center will no longer accept checks from you and you will be asked to pay in cash. 7. Payment plans can be arranged, at your request, if the need for such arrangements can be established. In the event it becomes necessary to use the courts to collect any unpaid balance, you agree to pay reasonable attorney fees and any and all court costs which may be incurred. I have received the Informed Consent for Services referenced on this page, as well as disclosure of my Health Insurance Portability and Accountability Act protections included in the Claret Center’s Notice of Privacy Practices. I agree to read the contract and to bring any questions about its contents or general concerns to my therapist’s attention at the following session. Client Name (Please Print) _____________________________ Date______________________________ Client Signature _________________________________________ Date_____________________________ Are you Pregnant? (Circle one) Yes/NO Witness __________________________________________________ Date ______________________________ Parent/Guardian_________________________________________ Date____________________________Witnessed _________________________________________________ Date_____________________________ 5536 S. Everett Avenue Chicago, IL 60637 Phone (773) 643-6259 www.claretcenter.org