To do
advertisement

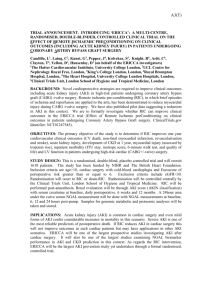
Effect of Remote Ischaemic preConditioning on clinical outcomes in patients undergoing Coronary Artery Bypass Graft surgery (ERICCA study): A multicentre randomised controlled clinical trial DJ Hausenloy, C Liang, Tim Clayton, G Kunst, S Kolvekar, J Pepper, DM Yellon Background: Given the increasing number of higher-risk patients undergoing cardiac surgery, there is an urgent need to develop novel cardioprotective strategies to reduce myocardial injury, preserve left ventricular function and improve clinical outcomes in this patients group. We have recently demonstrated in a proof-of-concept clinical study comprising 56 patients that remote ischaemic preconditioning (RIC)1, using brief ischaemia and reperfusion applied to the upper limb using a blood pressure cuff is able to reduce myocardial injury (43% reduction in troponin-T) in patients undergoing elective cardiac surgery at the Heart Hospital 2. We have gone to demonstrate that patients undergoing cardioprotection using cold-blood cardioplegia alone also benefit from RIC 3. Other groups have demonstrated that the RIC stimulus can reduce myocardial injury in children undergoing corrective cardiac surgery for congenital heart disease 4, in patients undergoing surgery for repair of an abdominal aortic aneurysm 5;6, and in patients undergoing elective percutaneous coronary intervention 7. We now intend to determine in a large multi-centre clinical study whether RIC using brief upper-limb ischaemia is able impact on short-term and long-term clinical outcomes in patients undergoing high-risk cardiac surgery. Hypothesis: Remote ischemic preconditioning using brief limb ischaemia/reperfusion will improve short-term and long-term clinical outcomes at one year in patients undergoing high-risk cardiac surgery. Primary outcome measure: Major adverse cardiac and cerebrovascular events (MACCE- death from any cause, stroke, myocardial infarction, or repeat revascularization) at one year. Secondary outcome measures: 1. Peri-operative myocardial injury over 72 hrs (serum CK-MB/Troponin-T or I 0,6,12,24,48,72). 2. Length of ITU/hospital stay, Inotrope score. 3. Peri-operative renal injury (blood NGAL) 5 samples over 3 days (0, coming off bypass, 12, 24, 48 hours) and incidence of Acute Kidney Injury (AKI). Daily creatinine for hospital stay, 6 weeks and one year. Hourly urine volumes on ITU and daily urine volumes thereafter. 4. 6 minute walk test at baseline and at 6 weeks and 12 months. 5. Quality of life at baseline, 6 weeks, 3, 6, 9, and 12 months. Substudy (140 patients): Left ventricular ejection fraction (echo) at baseline, 6 weeks and one year. (a) Research Design: Multi-centre double-blind randomised controlled clinical trial. (b) Study Population: High-risk patients (defined by additive Euro-SCORE≥6) undergoing elective CABG±valve surgery with cold-blood cardioplegia. (c) Planned Interventions: Remote ischaemic preconditioning (RIC) comprising four 5 min cycles of inflation (to 200mmHg) and deflation of a cuff placed on upper arm. Sham RIC will comprise four 5 min cycles of inflation (to 40mmHg) and deflation of a cuff placed on upper arm. (d) Proposed outcome measures: Primary outcome: Major adverse cardiac (Death, myocardial infarction, revascularisation) and cerebrovascular events (stroke) or MACCE at one year. Secondary outcomes: Perioperative myocardial and renal injury; Length of ITU/hospital stay and inotrope score; Left ventricular ejection fraction and 6 minute walk test at baseline, 6 weeks and one year (subgroup analysis); Quality of life at baseline, 6 weeks, 3 months 6 months, 9 months, and one year. (e) Assessment and follow up: Outcome measures will be assessed from the patient GP and medical notes, postal surveys, and 6 week and one year outpatient appointments. Safety will be assessed using a Standard Operating Procedure. 1 (f) Proposed sample size: We plan to recruit 1606 patients through 12 surgical centres. RIC reduced myocardial injury as measured by troponin-T by 43% in elective CABG surgery patients (EuroSCORE mean 3.0)2. In the recently published SYNTAX study the major adverse cardiac and cerebrovascular events (MACCE- death from any cause, stroke, myocardial infarction, or repeat revascularization) event rate was 12.4% of patients at 12 months following CABG surgery8. To detect a 35% reduction in this primary endpoint in the RIPC-treated group (from 12.4% to 8.06%), with a power of 80% and a significance level of 5%, a sample size of 765 patients will be required for each trial arm (1530 in total). To allow for dropouts (5% as per SYNTAX study) we plan to recruit 1606 patients in total. It should be noted that our patients will be highrisk (as defined by additive EuroSCORE≥6), and in the SYNTAX study the patient population was low risk with a mean EuroSCORE of 3.8±2.6. Echo substudy: In a previous study, ischaemic postconditioning (an endogenous cardioprotective strategy similar to RIC) has been reported to improve LV ejection fraction by 14.2% (relative increase) from 49% to 56% at one year in ST-elevation myocardial infarction patients 9. The mean difference would thus be 7% with a pooled SD of 10.5. To demonstrate such a difference as being statistically significant at the 5% level, with 90% power, requires 48 subjects per group (96 in total). We plan to recruit 140 patients from a single site. (g) Statistical analysis: Survival analyses will be carried out for clinical endpoints. MACCE; hazard ratios and confidence intervals will be calculated using Cox’s proportional hazards modelling. All analyses will be carried out on an intention to treat basis. There is no planned interim analysis. There is a planned subgroup analysis of LV ejection fraction. (h) Project timetables including recruitment rate: The planned duration of the study will be 48 months: (1) 0-6 months-Study preparation; (2) 6-30 months-Patient recruitment; (3) 18-42 months- 1 year follow-up; (4) 42-48 months- Assessment of clinical outcomes and cost-effectiveness, data analysis, writing-up and dissemination of research findings. Over the 24 month recruitment period we would expect to recruit about 134 high-risk CABG patients through each of the 12 recruiting centres, which equates to 1.7 patients per week from each centre. Each centre operates on about 7-10 high-risk surgical patients per week, meaning that we would have to recruit at least 25% of the eligible patients. (i) Cardiac surgery centres 1. UCLH Heart Hospital 2. Golden Jubilee Hospital 3. Royal Brompton Hosp 4. Harefield Hospital 5. King’s College Hospital 6. Papworth Hospital 7. Hammersmith Hospital 8. St Thomas Hospital 9. St Bart’s Hospital 10. London Chest Hospital 11. Essex CTC 12. Royal Sussex,Brighton 13. Wolverhampton Hospital 14. Edinburgh Royal Infirmary 15. Bristol Royal Infirmary 16. Manchester Royal Infirmary Shyam Kolvekar Geoff Berg John Pepper John Pepper Jatin Desai David Jenkins Prakash Punjabi Chris Blauth Rakesh Uppal Rakesh Uppal Andrew Ritchie Uday Trivedi Moninder Bhabra Renzo Pessotto Raimondo Ascione Dan Keenan Trial Steering Committee (TSC) Prof Sir David Taggart (independent chair) Two Service Users (two previous CABG±valve patients) Prof Derek Yellon, Dr Derek Hausenloy, Dr Shyam Kolvekar, Prof John Pepper, Prof Michael Marber, Prof Liam Smeeth, Dr Gudrun Kunst, Dr Chris Laing, Dr Luciano Candilio, Mr Tim Clayton and Ms Rosemary Knight. Trial Management Group (TMG) Dr Derek Hausenloy, Mr Tim Clayton, Ms Rosemary Knight, Mr Steve Robertson. Data and Ethics Monitoring Committee (DMEC) Dr Rajesh Kharbanda, Mr Adrian Marchbank,Prof Jean Morris. 2 Flow diagram ERICCA: Overview Enrollment High-risk patients (EuroSCORE≥6), CABG valve surgery, cold blood cardioplegia Analysis Follow-up Allocation Pre-admission clinic : Baseline blood tests, 6 min walk test, echo and HRQOL assessment. Patients randomised on am of surgery (N= ) Allocated to RIC treatment arm (N= ) Blood pressure cuff used to apply RIC protocol Bloods taken for Trop-T/I at 0,6,12,24,48,72 hrs NGAL Patient reviewed in OPA clinic at 6 weeks (N=) HRQOL at 3, 6, 9 mths (N=) Patient reviewed in research OPA at 1 year (N=) Patient data analysed at one year (N= ) Excluded from analysis (N= ) Allocated to control arm (N= ) Un-inflated cuff placed on arm as control protocol Bloods taken for Trop-T/I at 0,6,12,24,48,72 hrs NGAL Patient reviewed in OPA clinic at 6 weeks (N=) HRQOL at 3, 6, 9 mths (N=) Patient reviewed in research OPA at 1 year (N=) Patient data analysed at one year (N= ) Excluded from analysis (N= ) References 1. Hausenloy DJ, Yellon DM. Remote ischaemic preconditioning: underlying mechanisms and clinical application. Cardiovasc Res. 2008;79:377-386. 2. Hausenloy DJ, Mwamure PK, Venugopal V, Harris J, Barnard M, Grundy E, et al. Effect of remote ischaemic preconditioning on myocardial injury in patients undergoing coronary artery bypass graft surgery: a randomised controlled trial. Lancet. 2007;370:575-579. 3. Venugopal V, Hausenloy DJ, Ludman A, Di Salvo CM, Kolvekar S, Yap J, et al. Remote Ischaemic preconditioning reduces myocardial injury in patients undergoing cardiac surgery with cold blood cardioplegia:a randomised controlled trial. Heart. 2009. 4. Cheung MM, Kharbanda RK, Konstantinov IE, Shimizu M, Frndova H, Li J, et al. Randomized controlled trial of the effects of remote ischemic preconditioning on children undergoing cardiac surgery: first clinical application in humans. J Am Coll Cardiol. 2006;47:2277-2282. 5. Ali ZA, Callaghan CJ, Lim E, Ali AA, Nouraei SA, Akthar AM, et al. Remote ischemic preconditioning reduces myocardial and renal injury after elective abdominal aortic aneurysm repair: a randomized controlled trial. Circulation. 2007;116:I98-105. 6. Walsh SR, Boyle JR, Tang TY, Sadat U, Cooper DG, Lapsley M, et al. Remote ischemic preconditioning for renal and cardiac protection during endovascular aneurysm repair: a randomized controlled trial. J Endovasc Ther. 2009;16:680-689. 7. hoole SP, Heck PM, Sharples L, Khan SN, Duehmke R, Densem CG, et al. Cardiac Remote Ischemic Preconditioning in Coronary Stenting (CRISP Stent) Study: a prospective, randomized control trial. Circulation. 2009;119:820-827. 8. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961-972. 9. Thibault H, Piot C, Staat P, Bontemps L, Sportouch C, Rioufol G, et al. Long-term benefit of postconditioning. Circulation. 2008;117:1037-1044. 3