Medical History Form - Advanced Dermatology Skin & Surgery
advertisement

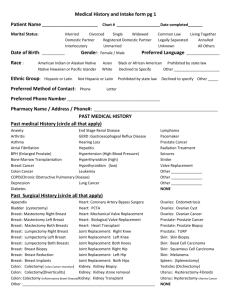
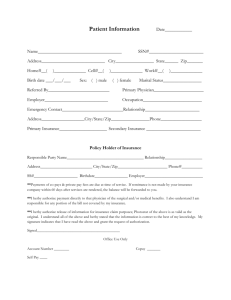
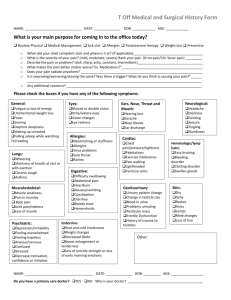
Advanced Dermatology and Skin Surgery MEDICAL HISTORY FORM PATIENT to please fill out: NAME: _________________________________________________ DATE: _________ BIRTHDATE:___/___/___ REFERRED BY: _________________________________________________________________________________ LIST OF CURRENT DR. & SPECIALISTS ___________________________________________________________ ALLERGIES: (DRUG, SEASONAL, AND FOOD ALLERGIES) _________________________________________ PHARMACY NAME/LOCATION: ________________________________________________________________ MEDICAL HISTORY: (Check the following medical conditions that you currently have) Anxiety Depression Leukemia Arthritis Diabetes Lung Cancer Asthma End Stage Renal Disease Lymphoma Atrial Fibrillation (Irregular Heartbeat) GERD (Reflux Disease) Pacemaker/Defibrillator Bone Marrow Transplantation Hearing Loss Prostate Cancer BPH (Benign Prostatic Hyperplasia) Hepatitis Radiation Treatment Breast Cancer Hypertension (High Blood Pressure) Seizures Colon Cancer Hypercholesterolemia (High Cholesterol) Stroke/TIA Pulmonary Disease/COPD HIV / AIDS Coronary Artery Disease/Heart Disease Hyperthyroidism Hypothyroidism Other (Please List) ___________________________________________________ PAST SURGERIES: Appendix (Appendectomy) Heart: Transplant Prostate: Prostate Cancer Bladder (Cystectomy) Joint Replacement Knee Date:____R or L Prostate: Prostate Biopsy Breast: (Mastectomy) Joint Replacement Hip Date:____R or L Prostate: TURP Breast: Lumpectomy (Right/Left/Both) Kidney: Kidney Biopsy Rectum: Rectal Resection APR Breast: Breast Biopsy Kidney: Kidney Nephrectomy Rectum: Rectal Resection Colon (Colectomy) Colon Cancer Resection Kidney: Kidney Stone Removal Skin: Skin Biopsy Colon (Colectomy) Diverticulitis Kidney: Kidney Transplant Skin: Basal Cell Carcinoma Colon (Colectomy): IBS Liver: Liver Transplant Skin: Squamous Cell Carcinoma Colon Colostomy Liver: Liver Shunt or Hepatectomy Skin: Melanoma Gallbladder (Cholecysectomy) Ovaries: Endometriosis Spleen: (Spenectomy) Heart: Coronary Artery Bypass Surgery Ovaries: Ovarian Cyst Testicles: (Orchidectomy) Heart: PTCA Ovaries: Ovarian Cancer Uterus(Hysterectomy):Uterine Cancer Heart Mechanical Valve Replacement Ovaries: Tubal Ligation Uterus(Hysterectomy):Cervical Cancer Heart: Bilogical Valve Replacement Pancreas: Pancreatectomy Uterus(Hysterectomy):Fibroids Other________________________________________________________ SKIN DISEASE HISTORY: Have you had any of the following skin conditions: Acne Dry Skin Poison Ivy Actinic Keratoses Eczema Precancerous Moles Asthma Flaking or Itchy Scalp Psoriasis Basal Cell Skin Cancer Hay Fever/Allergies Squamous Cell Skin Cancer Blistering Sunburns Melanoma Other: ____________________________________________________________________________________ Do you wear Sunscreen? Yes or No PAGE 1 TURN OVER If yes, what SPF? ____________ Do you tan in a tanning salon? Yes or No FAMILY HISTORY: Do you have a family history of Melanoma? Yes or No If yes, which relative?___________________________ Do you have a family history of: Autoimmune Disorder Carcinoma: Basal Cell Carcinoma: Squamous cell Diabetes Eczema Psoriasis Hair Loss Hay fever/Asthma Other Cancer/Malignancy (Please mark which relative & listed condition) Mother____________ Daughter______________ Nephew____________ Grandmother_______________ Father_____________ Son__________________ Niece______________ Grandson___________________ Sister______________ Uncle________________ Grandfather______________ Granddaughter________________ Brother_____________ Aunt_________________ Other: __________________________________ SOCIAL HISTORY: Occupation: _______________________ Place of Employment:________________________________ If Retired: Previous Occupation:____________________________________________ Social History Details Currently Smokes Has smoked in the past Smokes Every Day Never Smoked Smokes few times per week Drug/Alcohol Use Type: ____________________ How Often?____________________________ Exercise: 1 time per day Few times per week Few times per month Never Exercise REVIEW OF SYSTEMS: Cardiovascular: Pacemaker Artificial Heart Valve Allergic / Immunologic: Premedication prior to procedures Allergy to lidocaine Endocrine: Pregnant or planning a pregnancy Gastrointestinal: GI Upset with Antibiotics Integumentary/Skin: Problems with Healing Changing Mole Defibrillator Artificial joints w/in past two years Rapid heartbeat with epinephrine Chest Pain Allergy to adhesive Immunosuppression Constitutional / Symptom: Yeast infections w/antibiotics Hematologic / Lymphatic: Problems with bleeding Allergy to topical antibiotic ointments Fever or Chills Unintentional Weight Loss Problems with scarring (hypertrophic or keloid) Rash PATIENT to please fill out: Please provide your complete list of Current Medications (including aspirin, herbals, vitamins – DOSAGE NECESSARY): Medication Dosage Reason _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________ _________________________ ___________ ____________________________________