Vitamin E

Current Opinion in Gastroenterology
Nonalcoholic Fatty Liver Disease: New
Treatments
Timothy Hardy, Quentin M. Anstee, Christopher P. Day
Disclosures
Curr Opin Gastroenterol. 2015;31(3):175-183.
Abstract and Introduction
Abstract
Purpose of review Nonalcoholic fatty liver disease is the most common cause of liver dysfunction in the western world because of its close association with obesity, insulin resistance and dyslipidaemia.
Nonalcoholic steatohepatitis (NASH) is a particular health concern due to the increased morbidity and mortality associated with progressive disease. At present, without specific targeted pharmacological therapies, the mainstay of therapy remains weight loss through dietary modification and lifestyle change; thus, the purpose of this review is to summarize the recent evidence for current and emerging therapies in
NASH.
Recent findings Some existing medications, including pioglitazones and angiotensin receptor antagonists, may be repurposed to help treat this condition. Vitamin E may improve histology in NASH, but safety issues limit its use. Recently, a number of novel agents specifically targeting nonalcoholic fatty liver disease pathogenesis have entered clinical trials, including the farnesoid X receptor agonist obeticholic acid, which has shown significant histological improvements in steatohepatitis and fibrosis.
Summary Diet/lifestyle modification remains the mainstay of treatment. For patients with NASH and advanced fibrosis, current liver-directed pharmacotherapy with vitamin E and pioglitazone offer some benefits; obeticholic acid appears promising and is currently being tested. Comorbidities must be diagnosed and treated; cardiovascular disease remains a primary cause of death in these patients.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of liver dysfunction in the western world [1] because of its close association with obesity, insulin resistance and dyslipidaemia; it is therefore considered the hepatic manifestation of the metabolic syndrome. A particular health concern is patients with nonalcoholic steatohepatitis (NASH) with accompanying hepatocellular injury that can lead to progressive liver fibrosis, cirrhosis and hepatocellular carcinoma (HCC) as well as increased cardiovascular risk.
[1] At present, there is no approved therapy for NASH and the optimal treatment remains uncertain; effective therapies are thus a research priority to reduce the anticipated burden of liver disease.
Therapy
The rationale for therapeutic approaches is centred on the concept that while simple steatosis has not been associated with morbidity, NASH is associated with a more than 10-fold increased risk of liver-related death (2.8 vs. 0.2%) and a doubling of cardiovascular risk; [2] at the time of diagnosis, 25
–33% of patients with NASH have advanced fibrosis, including cirrhosis.
[3,4] After adjustment for confounders, NASH has a similar fibrotic potential to that of chronic hepatitis
C.
[3,4] Pooled data suggest that about 21% of patients with NASH will have some regression of fibrosis while 38% of patients will progress over 5.3 years' followup, [3] results that have recently been confirmed in a dual-biopsy Northern
European population.
[5]
Lifestyle Modifications
Weight reduction is recommended as the initial step in management of NASH.
Pharmacological agents such as orlistat may help achieve weight loss; however, whether these confer additional independent benefit beyond that due to weight loss is unclear.
[6,7] Lifestyle modification therefore remains the primary therapy for weight reduction, particularly in the absence of approved pharmacotherapy; it encompasses diet, physical activity (aerobic and resistance) and behavioural change, or a combination of all three. Trial evidence shows that weight reduction more than 7% sustained over 48 weeks is associated with significant reduction in histological severity of NASH.
[8] A systematic review of the available evidence for lifestyle modifications in NAFLD has recently been conducted.
[9] Less than 50% of patients achieve the necessary weight loss goal of more than 7% in the trial setting, [8] and many have questioned the sustainability of this type of intervention.
[10] Resistance training, which is less burdensome on the cardiovascular system, shares the metabolic improvements seen in more strenuous aerobic exercise and may be more sustainable.
[11] Nevertheless, in the many patients that fail to implement lifestyle changes or have advanced disease (bridging fibrosis) on index biopsy, specific liver-directed pharmacotherapy may be needed. No drugs are currently licensed specifically for treating NASH; there is an urgent need for well designed randomized controlled trials (RCTs) with appropriate endpoints to narrow this gap. Table 1 [12 –21,22,23–25] summarizes the current evidence for therapies in NASH.
Therapies of Potential Value for the Treatment of Nonalcoholic
Steatohepatitis
Very few large RCTs have been published on which evidence-based treatment for NASH is recommended. Therapies with potential benefit in NASH include thiazolidinediones (TZDs) and vitamin E.
Thiazolidinediones
The most extensively studied and for which the best data are available is for the use of TZDs in the treatment of NASH.
[4] Central to their action is their ability to ameliorate insulin resistance and promote fatty acid uptake peripherally; [26] free fatty acids are thus diverted away from the liver towards adipose tissue.
TZDs activate the master adipocyte differentiation regulator, peroxisome proliferator-ac tivated receptor (PPAR)γ, allowing transdifferentiation of preadipocytes into insulin-sensitive, fat-storing adipocytes.
[27 –29] Interestingly,
PPARγ ligands also attenuate liver fibrosis by suppressing the transdifferentiation of hepatic stellate cells into activated myofibroblasts suggesting an additional direct hepatoprotective effect.
[30 –32] They also have antiinflammatory effects [33] and increase circulating adiponectin, an antisteatogenic and insulin-sensitizing adipokine.
[34,35]
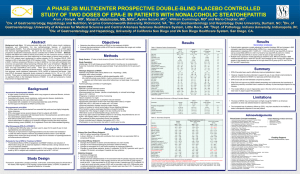
The largest multicentre RCT to date included 247 nondiabetic noncirrhotic patients with biopsy-proven NASH who received pioglitazone (30 mg/day), vitamin E (800 IU/day) or placebo for 96 weeks. Histological improvement that included a reduction of two points in the NAFLD activity score (NAS) with no worsening of fibrosis was the primary endpoint; pioglitazone failed to achieve a statistically significant effect compared with placebo.
[12] However, it did significantly improve each individual component of the NAS score (steatosis, lobular inflammation and ballooning). When the analysis was confined to patients with definite steatohepatitis on their index biopsy, pioglitazone achieved the primary endpoint. Several other well conducted trials have shown improvements in steatosis, necroinflammation and ballooning; [36 –38] however, to date, no study has shown a definite improvement in fibrosis, which is not surprising given the relatively short follow-up periods in most studies. TZDmediated effects seem to be abrogated upon treatment discontinuation; at 3 months, alanine transaminase (ALT) and homeostatic model assessment return to baseline. In seven out of nine patients who discontinued medication, recurrent NASH was seen at a 48-week posttherapy biopsy.
[39]
Unfortunately, side-effects (weight gain, [40] bone loss/fracture risk, [41] increased risk of myocardial infarction with rosiglitazone, [13] increased risk of bladder cancer with pioglitazone [14] ) and the possible need for long-term therapy [39] have
limited widespread acceptance, with rosiglitazone withdrawn from the market in most countries. Pioglitazone remains available and current guidelines suggest consideration in older patients with biopsy-proven advanced fibrosis that are unable to adopt or maintain lifestyle intervention, with continued metabolic risk factors; caution is required in patients with diabetes or those with heart failure.
[4,42]
Vitamin E
Apart from targeting aspects of the metabolic syndrome that may have beneficial liver effects, liver-specific therapies have also been investigated in
NASH. The role of oxidative stress in disease pathogenesis, in particular, has initiated several studies of antioxidants, primarily vitamin E. Vitamin E consists of eight tocopherols; α-tocopherol is the most active. Its presence in the phospholipid bilayer of cell membranes allows prevention of the nonenzymatic oxidation of cell constituents by free radicals. Vitamin E may also inhibit profibrotic activity [43,44] and downregulates nuclear factor (NF)-
κB-mediated inflammatory pathways in the liver.
[45] Preclinical in-vitro and in-vivo studies have shown that in two fibrosis models, vitamin E can ameliorate liver injury blocking both apoptotic pathways and mitochondrial toxicity.
[46,47]
The Pioglitazone versus Vitamin E versus Placebo for the Treatment of
Nondiabetic Patients with Nonalcoholic Steatohepatitis (PIVENS) trial, described earlier, is the largest and most recent study comparing pioglitazone and vitamin E at 800 IU/day to placebo in nondiabetic, noncirrhotic patients; it reported that vitamin E improved all histological lesions in NAFLD except for fibrosis, and patients taking vitamin E had a greater than two-point improvement on NAS score significantly more often compared with placebo.
[12] A pilot study suggested that pioglitazone and vitamin E are superior to pioglitazone alone but the study was not appropriately powered.
[48] The positive and encouraging results seen in adult NAFLD may not extrapolate to paediatric NAFLD. The largest trial of vitamin E in paediatric NAFLD, the Treatment of NAFLD in
Children (TONIC) trial, randomly assigned children and adolescents to receive vitamin E (800 IU/day) vs. metformin (1 g/day) or placebo for 2 years. Vitamin E significantly improved hepatocyte ballooning but not lobular inflammation, steatosis nor fibrosis. The primary endpoint of reduction in ALT levels, more often than placebo, was not met.
[16]
The results of these studies with vitamin E need to be balanced against the emerging body of data that vitamin E may increase all-cause mortality: an
additional 39 deaths per 10 000 people for those on high-dose (400 IU/day) vitamin E in a dose-dependent manner starting at 150 IU/day, much less than the doses trialled in NASH.
[15] Furthermore, vitamin E therapy may be associated with an increase in prostate cancer in men above 50 years old according to a large study of 35 000 patients, and a 20% increased risk of haemorrhagic stroke.
[49,50] In light of these risks, the current American
Association for the Study of Liver Diseases guidelines recommend that use of vitamin E may be considered in nondiabetic adults with NASH, but not diabetic patients or children.
[28]
Therapies With No Clear Benefit
Several well recognized pharmacotherapies have been investigated in NASH; currently, they are not recommended for its treatment.
Metformin
Although metformin initially seemed promising in animal models of NASH, [51] no histological improvement in steatohepatitis has been shown in RCTs in adult and paediatric NASH.
[16,17] Low-dose metformin could not mitigate the weight gain associated with rosiglitazone in a recent RCT, [52] although its effect seems likely to be through weight loss in the small number of treated patients.
[53] As it has no effect on histology, metformin is not currently recommended as a targeted treatment for NAFLD.
Statins
Statins are well recognized in the treatment of dyslipidaemia, but their use as a specific treatment for NAFLD is not well evidenced. Data from the Greek
Atorvastatin and Coronary Heart Disease Evaluation study did, however, demonstrate a fall in ALT levels with atorvastatin [19] and the St Francis Heart
Study showed a reduction in steatosis radiologically with 20 mg daily of atorvastatin combined with vitamins C and E.
[18] There are, however, no histological data currently available to support the use of atorvastatin for
NAFLD. Although histological data exist for simvastatin, in a trial of 10 patients with biopsy-proven NASH, there was no statistically significant improvement in serum liver enzymes, hepatic steatosis, necroinflammatory activity or stage of fibrosis within or between treatment and placebo.
[20] However, its use to reduce cardiovascular risk in patients with NAFLD is clear and there is no evidence to suggest that patients with NAFLD are at increased risk of statin-related liver injury.
[54]
Ursodeoxycholic Acid
Ursodeoxycholic acid (UDCA), by preventing apoptosis and downregulating inflammatory pathways, is an example of a potential cytoprotective agent investigated in NASH. The largest study to date comparing UDCA and placebo showed an unanticipated improvement in the placebo arm, making the effect of the drug hard to interpret.
[55] A Cochrane review of four randomized trials using
UDCA showed no significant improvement in liver function tests and histological data were lacking.
[21] Until there is evidence of clear histological benefit, UDCA cannot be currently recommended for NASH.
Polyunsaturated Fatty Acids
Despite preliminary da ta from small studies suggesting that ω-3 polyunsaturated fatty acid supplementation reduces liver fat content, [23] a large trial testing two doses of ethyl-eicosapentaenoic acid did not show any histological efficacy.
[22]
Therapies With Unclear Benefit
Some agents tested in NASH have robust preclinical data, but are yet to be investigated in large RCTs.
Angiotensin Receptor Blockers
Angiotensin receptor blockers are well established in the treatment of hypertension, a second key component of the metabolic syndrome.
Experimental work has clearly shown that angiotensin II promotes survival of hepatic myofibroblasts by activation of IκB kinase-mediated phosphorylation of
NFκB subunit RelA.
[56] A small pilot study of seven patients with NASH treated with losartan for 48 weeks showed improvements in necroinflammation and fibrosis.
[24] Larger studies examining the utility of this agent are ongoing.
Pentoxifylline
Pentoxifylline (PTX) is a tumour necrosis factor-
α agonist and reduces production of oxygen-free radicals.
[57] Animal models have also suggested an antifibrotic effect together with significantly reducing steatohepatitis.
[58] The largest and most recent RCT published in 2011 included 55 patients with NASH receiving PTX or placebo; patients on PTX showed a mean 1.6-point improvement on the NAS score vs. 0.1 point in placebo. Although not significant, there was a slight improvement in fibrosis.
[25] Before PTX can be
recommended as primary therapy, larger and more compelling data are warranted.
Novel Approaches
New therapies with strong experimental evidence are currently being trialled in human NASH, and may provide hope of a targeted pharmacotherapy; these are summarized in Table 2 .
[59 –66]
Caspase Inhibition (GS-9450)
Preclinical models have shown that hepatocyte apoptosis is a hallmark of
NASH, [67] the extent of which correlates with disease severity. In a recent phase-
2 placebo-controlled trial, 124 patients with histologically characterized NASH were randomized to once-daily placebo or GS-9450, a selective caspase inhibitor, at varying dosages for 4 weeks. In the highest dose group (40 mg), both ALT and cytokeratin-18 fragment levels improved but only ALT reached significance; GS-9450 was safe and well tolerated.
[68]
PPAR Agonists (GFT-505)
GFT505 is a dual PPARα and PPARδ agonist that in animal models of dietaryinduced NASH has shown a reduction in steatosis, inflammation and proinflammatory genes; interestingly, GFT-505 has also demonstrated antifibrotic properties, independent of metabolic abnormalities.
[69] Human studies have shown that GFT-505 improves liver function tests, dyslipidaemia and insulin sensitivity in obese, insulin-resistant patients.
[70,71] A phase 2b RCT is now ongoing based on these encouraging results.
[60]
Farnesoid X Receptor Agonists (Obeticholic Acid)
Bile acids act as metabolic signalling molecules, aiding dietary lipid absorption, and are involved in cholesterol homeostasis; they are reabsorbed into the enterohepatic circulation and direct hepatic triglyceride and glucose metabolism. They activate nuclear hormone receptor farnesoid X receptor
(FXR) and the G protein-coupled cell surface receptor transmembrane G protein-coupled receptor, which inhibit hepatic de-novo lipogenesis, hepatic gluconeogenesis and glycogenolysis and improve insulin sensitivity. In animal studies, FXR activation has anti-inflammatory actions, partly by inhibiting NF-
κB.
[72,73] In-vivo evidence exists for a protective effect of FXR agonists against liver inflammation and fibrosis in the methionine
–choline-deficient model of
NASH.
[74] Thus, obeticholic acid, an FXR agonist, was studied in a small pilot
trial of 23 diabetic patients with NAFLD. Patients received 6 weeks of the study drug at either 25 mg or 50 mg daily or placebo. Patients on the study drug lost weight with an associated fall in serum γ-glutamyl transferase and an improvement in the noninvasive Enhanced Liver Fibrosis panel observed more often than in the placebo group.
[75]
A 72-week trial of 273 patients with NASH randomized to obeticholic acid or placebo has recently reported evidence of significant reductions in histologically defined endpoints including degree of steatosis, grade of inflammation/ballooning degeneration and stage of fibrosis.
[76] These changes were accompanied by mild weight loss and improved clinical biochemistry parameters, also consistent with reduced liver injury. However, a rise in total cholesterol and a disadvantageous change in high-density lipoprotein/lowdensity lipoprotein ratio were also observed with obeticholic acid treatment.
[76] Despite this, the agent remains one of the first in which robust, beneficial changes in liver histology have been identified.
Other promising agents with anti-inflammatory, antifibrotic or insulin-sensitizing properties currently in development or undergoing testing in RCTs in NASH include dual C –C chemokine receptor 2/5 antagonists, glucagon-like peptide-1 agonists, dipeptidyl peptidase-4 inhibitors and anti-lysyl oxidase-like 2 antibodies (simtuzumab).
Hepatocellular Carcinoma
Obesity and diabetes have been well established as risk factors for HCC.
[77 –
79] Recently, HCC has been linked to NAFLD, [80] and there is mounting evidence that the same PNPLA3 genetic variant (I148 M, rs738409) that has long been associated with progressive NAFLD also confers an increased risk of NAFLD-
HCC.
[81,82] The prevalence of HCC in cirrhotic NAFLD remains undetermined, [83] although steatohepatitis was identified as the underlying aetiology in 24% of patients in a series of HCC surpassing all other causes of chronic liver disease [70] and this trend is set to increase further. In the United
Kingdom, a more than 10-fold increase in NAFLD-associated HCC has been observed from 2000 to 2010, with NAFLD-HCC accounting for 34.8% of all HCC cases.
[84] It is increasingly recognized that NAFLD is a cause of noncirrhotic
HCC. A recent Japanese cross-sectional study analyzed 87 cases of HCC occurring in patients with histologically characterized steatohepatitis; no established cirrhosis was demonstrated in 43 cases.
[85] Most worryingly, HCC has been reported in patients even without steatohepatitis.
[86] An analysis of a
US insurance claims database found NAFLD was the leading condition associated with HCC, with cirrhosis reported in just 46% of these cases.
[87]
Adipose tissue expansion and subsequent release of proinflammatory cytokines/adipokines [88,89] and lipotoxicity [90] together promote insulin resistance; hyperinsulinaemia results in increased bioavailability of insulin growth factor-1, which further stimulates cellular proliferation and inhibits apoptosis.
[91] Metformin, a biguanide that activates adenosine monophosphate-activated protein kinase and has antiproliferative effects has been shown to inhibit hepatocyte proliferation and induce cell-cycle arrest in hepatoma cell lines.
[92] Consequently, targeting insulin resistance with metformin has been investigated in observational and case –control studies of HCC.
[93,94] Among patients with type 2 diabetes mellitus, metformin was associated with an estimated 62% reduction in the risk of HCC in a recent meta-analysis (odds ratio, 0.38; 95% confidence interval, 0.24
–0.59).
[95] However, the ability of metformin to protect against
NASH-associated carcinogenesis is not firmly established as human data are retrospective and do not mitigate against treatment assignment bias.
There is biological plausibility that statins reduce cancer risk via HCC-specific
(Myc inactivation) [96,97] as well as antiproliferative, proapoptotic, antiangiogenic, immunomodulatory and antiinfective mechanisms.
[98 –100] A recent meta-analysis examining over 1.4 million patients found results to be heterogeneous.
[101] Data from observational studies indicated that statins lowered the risk of HCC in various patient populations; however, no clear benefit was found when only rigorously conducted RCTs were included in the analysis.
[101]
Bariatric Surgery
Surgical weight loss interventions have been investigated in the treatment of
NAFLD; the most common procedures tested are laparoscopic adjustable gastric banding and Roux-en-Y gastric bypass. Several uncontrolled studies have reported that bariatric surgery has shown to produce significant weight loss and may be beneficial for the treatment of NAFLD, [102,103] but the lack of
RCTs precluded this conclusion in a Cochrane review.
[104] Nevertheless, a recent study reported that on postbariatric biopsy of 160 patients, steatosis resolved in 75% and steatohepatitis resolved in 90%. Fibrosis of any grade resolved in 53% of patients, with even bridging fibrosis resolved in 29% of patients.
[105] The effects of bariatric surgery on steatosis and ballooning appear durable in a 5-year sequential biopsy study, but fibrosis worsened significantly,
although more than 95% of patients had a fibrosis score F1 or less at 5 years.
[106] Clearly, surgical intervention is not a panacea for all patients with
NASH, and more robust data from RCTs are needed before recommendations can be made.
Conclusion
Despite its prevalence and rising incidence, NAFLD is marked by substantial interpatient variability in prognosis and continues to lack the breadth of therapeutic research and development shared by other causes of chronic liver disease. Although major advances have been made in understanding pathogenesis and also identification of genetic modifiers of liver injury extending beyond simple steatosis including PNPLA3 and TM6SF2 , [81,107,108] these advances have not yet been fully capitalized upon and so we lack effective pharmacotherapy. Diet and lifestyle modification remain the mainstay of treatment. For patients with NASH and advanced fibrosis, current liver-directed pharmacotherapy with vitamin E and pioglitazone offer some benefits in selected cases. Figure 1 provides a schematic of treatment, once the diagnosis of NASH has been made. However, the beneficial effects of these therapies must be balanced with the potential adverse effects, limiting their widespread use. Coexisting comorbidity must be diagnosed and treated because CVD remains primary cause of death in these patients. The new agents currently in trial provide the first hope of effective, targeted pharmacotherapy in this field.