Referral Checklist for Autism
advertisement

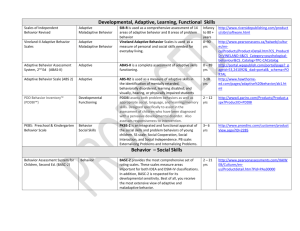
Referral Checklist for Autism Student’s Name ____________________________ Date sent to psych services* __________________ _____ Parent Input Form _____ SST Meeting Summary & Intervention Plan _____ SST Behavioral Supports Form (if applicable) _____ Behavior Intervention Plan (if applicable) _____ SST Follow-up Meeting Summary (if applicable) _____ Permission to test with Prior Written Notice _____ Student Support and Interventions Team Referral for Comprehensive Evaluation _____ General Education Teacher’s Input Form _____ Medical Information Form completed within the past year (A medical report by a licensed physician evaluating the possibility of other impacting health conditions is required) _____ Adaptive Behavior Evaluation Scale-Revised Second Edition School Version (ABES-R2 SV) completed by classroom teacher _____ Vineland-II Survey Interview Form completed in a direct interview with the parent OR for high functioning students the Adaptive Behavior Evaluation Scale-Revised Second Edition Home Version (ABES-R2 HV) _____ Autism Spectrum Disorder Evaluation Scale – School Version (ASDES SV) (Available upon request from the Educational Diagnostician) _____ Gilliam Autism Rating Scale – Third Edition (GARS-3) completed by parent/guardian (Available upon request from the Educational Diagnostician) _____ Speech/Language/Communication Skills Evaluation (A Speech/Language Specialist is a required member of the assessment team) o A functional communication assessment o Evaluation of phonology, morphology, syntax, semantics, and pragmatics *(Please do not send the referral file to psych services until all information has been gathered and included in the referral folder.)