Word 41KB
advertisement

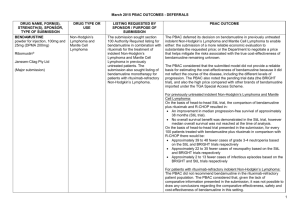
Appendix A to Item 11.03 Managed Access Programme framework following March 2015 PBAC. Framework for the Managed Access Programme for submissions to the PBAC The Managed Access Programme (MAP) is a mechanism that enables the Pharmaceutical Benefits Schedule (PBS) listing of products, under special circumstances of high unmet clinical need, on terms that allow for the resolution of otherwise unacceptable clinical or economic uncertainty for the Pharmaceutical Benefits Advisory Committee (PBAC). It seeks to enhance the quality and strength of evidence provided to decision-makers in reimbursement applications. Listing is in conjunction with, and linked to, the subsequent provision of more convincing evidence that is able to resolve specific existing areas of uncertainty as identified by the PBAC. The PBAC provides advice in relation to the initial sources of uncertainty and whether the evidence provided in the submission is sufficient to support initial listing under this programme until a final review of the additional evidence is completed at a predefined point in time. In most cases where there are not sufficient high quality data to clarify the efficacy and safety of a drug, randomisation in a Human Research Ethics Committee approved clinical trial is an appropriate standard of care. Such trials are not subsidised via the PBS. The application of the MAP mechanism is thus restricted to submissions where the PBAC agrees that, based on the data available, the proposed drug would provide a significant net clinical benefit, but the PBAC is uncertain about the magnitude of that benefit and therefore the price that should be paid, and when: there is a high and urgent unmet clinical need for the drug; the PBAC would not otherwise recommend the listing of the drug at the proposed price because the extent of the clinical effect is uncertain and/or there is a high cost to the PBS overall and/or on a per patient basis; and there is evidence that can reliably be reported and evaluated within a reasonable timeframe, which the PBAC is satisfied would resolve the identified area of uncertainty. MAPs are complementary to risk sharing agreements (RSAs) which address financial or budgetary uncertainty. MAPs, RSAs and special pricing arrangements (SPAs) are formalised in deeds of agreement. Managed Access Programme (MAP) parameters A submission for a MAP should be considered as an exception and not the rule and should meet the specified criteria below. A MAP may be initiated by a Sponsor as a proposal within a major submission or by a Sponsor, the PBAC or the DoH during the assessment and evaluation of a submission. MAP submissions may be appropriate where: the PBAC considers or has agreed that there is a high and urgent unmet clinical need for the proposed drug in the indication requested by the sponsor. The consideration of unmet clinical need would include an assessment of the prevalence 1 Appendix A to Item 11.03 Managed Access Programme framework following March 2015 PBAC. and severity of the disease, whether alternative therapies are available, and the extent to which the proposed drug is expected to meet the unmet clinical need; the PBAC is satisfied that new evidence will become available within a reasonable time frame that will resolve the issues of clinical and/or economic uncertainty that would otherwise have prevented an initial positive recommendation. The time frame should as far as possible be consistent with the standard term of Deeds of Agreement and any additional follow up beyond the standard term should be agreed at the time of initial listing; implementation is via a deed of agreement, as an administrative tool to ensure clear understanding by all parties of the obligations under the MAP framework and the consequences of potential outcomes from the additional evidence, and to ensure that the proposal, if adopted, is being used in conjunction with other existing tools designed to manage the entry of a new drug, as appropriate; and any subsequent review by the PBAC of the evidence specified by the deed of agreement would also include a consideration of all other relevant evidence at that time. Sponsor The major submission where the sponsor initiates consideration of a MAP would need to include the following: justification for the claim of high and urgent unmet clinical need; all evidence available at the time of the initial PBAC consideration, including evidence and rationale to support the validity of any surrogate outcomes used as the basis of the PBAC assessment where relevant; the areas of uncertainty (clinical and economic) as identified by the sponsor; extensive sensitivity analyses to illustrate the potential impact of the identified uncertainties on the initial incremental cost-effectiveness ratio (ICER); details of the proposed additional evidence, with a discussion by the sponsor of how such evidence would resolve the areas of uncertainty the sponsor or the PBAC had identified, including those in relation to the extent of the clinical or economic effect (or other circumstances in the future) which would be addressed in a subsequent submission to the PBAC; and anticipated timeframe for submission of the additional evidence. Where a MAP is suggested by the PBAC or is proposed for consideration during the evaluation of a product, the Sponsor must at a minimum provide: details of the proposed additional evidence and a discussion by the sponsor of how such evidence would resolve the identified areas of uncertainty, including those in relation to the extent of the clinical or economic effect; and the anticipated timeframe for submission of the additional evidence. 2 Appendix A to Item 11.03 Managed Access Programme framework following March 2015 PBAC. PBAC As part of the MAP submission evaluation process, the PBAC would consider the usual clinical and economic evidence available at the time of the initial consideration, and the additional information relevant to the provision of further evidence in a subsequent submission to the PBAC under the MAP framework. The PBAC would determine if a MAP is appropriate and accordingly, may: make a recommendation on listing and price based on the evidence available at the time of its initial consideration; identify its key areas of uncertainty for decision making (which may or may not be identical to the uncertainties identified in the submission by the sponsor where provided); and identify the evidence it requires to resolve the areas of uncertainty, the timeframe for submission of that evidence and the potential consequences of the evidence outcomes. Price While a future price cannot be specified or guaranteed at the time of the initial listing, the PBAC would consider the additional evidence in a subsequent submission and a price change taking into account the extent to which the uncertainties are resolved by the additional evidence. A deed of agreement would be established in all cases to record the possible consequences of the additional evidence on price. Disclosure of information At a minimum, the following information would be disclosed in the Public Summary Documents (PSDs): the identification of the proposed listing as a listing under the MAP and the consequences this may have for patients and any future competitors; the uncertainties identified at the time of the initial consideration by the PBAC; the PBAC-agreed description of the evidence required to address the area of uncertainty; and the anticipated timeframe for provision of the additional evidence to the PBAC. Further, a future PSD would be required, arising from PBAC deliberations relating to the additional evidence submitted according to the deed of agreement, and any other available evidence considered at that time by the PBAC. Patients who may be prescribed a drug subsidised under an MAP must, through their relevant prescribers, receive appropriate disclosure as to the circumstances of the drug being listed on the PBS. At a minimum, they must be informed why a drug is listed through a MAP and of the possibility that the drug may be delisted at the end of the MAP in which case they could elect to pay for the drug privately to continue treatment. If clinically appropriate, or recommended by the PBAC, patients and their prescribers must receive full disclosure (consistent with the informed consent requirements of a clinical trial) of the risks 3 Appendix A to Item 11.03 Managed Access Programme framework following March 2015 PBAC. involved in taking the drug, including the risk that the drug may not be as effective as anticipated, as well as the risk of unanticipated adverse events. Arrangements should be made to ensure a record of written acknowledgement that this information has been conveyed to and understood by each patient prescribed a drug via a MAP. If the MAP also requires that data be collected about PBS-subsidised patients, then the information to be collected must also be appropriately disclosed and written consent obtained from the patient. Not for disclosure If the company requests, the effective price of the drug would not be disclosed. Cost recovery The PBAC and its subcommittees would need to evaluate the new evidence provided in the further submission, and in this context, the subsequent submission would be treated as a major submission and an appropriate cost recovery process undertaken. Deed of agreement As part of the MAP process, there would be a deed of agreement which would specify items including: the agreed initial price; the areas of clinical and/or economic uncertainty as identified and specified by the PBAC that would need to be resolved by provision of additional evidence; the timeframe for submission of additional evidence and a statement of intent by the PBAC to consider the evidence within the accepted time frame; acknowledgment that there may be other areas of uncertainty yet to be identified which could impact on the initial ICER; agreement on how the additional evidence would be presented in updated clinical and/or economic evaluations, and how these evaluations could influence subsequent listing recommendations by the PBAC affecting restrictions, pricing and/or rebates; the expected consequences for pricing following the submission of the additional evidence via the MAP which acknowledges the need for a ‘confidence discount’ reflecting the reduced confidence in the initial evidence submitted to the PBAC, such as: o if the PBAC has recommended listing at a higher price than the PBAC considered was justified by the initial existing evidence, a mechanism needs to be available for payment of a retrospective rebate with interest to the Commonwealth should the submission of additional evidence show that the drug is failing to deliver on its claimed benefits; o if the PBAC has recommended listing at a lower price, that the PBAC considers is justified given the existing evidence, a mechanism needs to be available for recommendation of a higher price to be paid subsequently should the submission of additional evidence confirm that the drug is delivering on its claimed benefits; 4 Appendix A to Item 11.03 Managed Access Programme framework following March 2015 PBAC. other consequences of potential outcomes from the additional evidence, which may include amending or introducing restrictions on use of the drug or, if deemed necessary, full disinvestment via de-listing; specification of the rights and obligations for the Sponsor of the original drug in the event that an subsequent competitor drug is recommended by the PBAC for listing before the MAP is completed and where the subsequently recommended drug may materially alter the basis of the MAP (for example, the subsequently recommended drug has a lower price, is supported by more convincing evidence, or might be used alongside or in sequence with the original drug, thus confounding any data collected in the context of the original PBS listing for the MAP); commitment by the sponsor and the Commonwealth to disclose any confidential information to the Sponsor of the subsequently recommended drug that would or could have a material impact on the extent or value of the clinical or economic effect of the original drug listed under the MAP or its competitor. Competitors MAPs are not intended to discourage competition. A competing drug subsequently submitted to PBAC that might replace a drug already listed under a MAP could have the potential to alter the extent of future clinical need, however not the QALY gained of the original drug over its original comparator. However, data being collected to verify key aspects of the estimated QALY gained for the original drug under its MAP might be confounded by the listing of the competing drug. The pricing of the competing drug is a matter for the PBAC based on its usual criteria, including, but not limited to, the comparability of the two products given the reduced degree of confidence the PBAC had in the incremental QALY gain modelled for the original drug at the time of its recommendation. If the competing drug is recommended by the PBAC, then, under applicable criteria outlined in the deed, the original sponsor would share the relevant terms of the deed with the subsequent sponsor and the subsequent sponsor would be informed of these terms, including on a confidential basis as necessary. Summary In summary, a submission that would not normally be recommended for listing by the PBAC because of unacceptable clinical and economic uncertainty could be recommended under a MAP provided the MAP parameters are met. This would mean: earlier access to the drugs by patients; earlier access to a subsidised market for the sponsor whilst acknowledging that some form of confidence discount may be required in recognition that the initial evidence is less convincing; clear articulation of the evidence required to resolve the identified area of uncertainty and the consequences of potential outcomes from the additional evidence; 5 Appendix A to Item 11.03 Managed Access Programme framework following March 2015 PBAC. agreement by the PBAC to review a submission once the additional evidence becomes available and to reconsider the listing in light of the new evidence; appropriate sharing of risk. It is envisioned that relevant stand-alone process guidelines applicable to the MAP and/or an update to existing guidelines may follow on from this framework. 6