Biopsychosocial History Form - Open Arms Psychological Services
advertisement

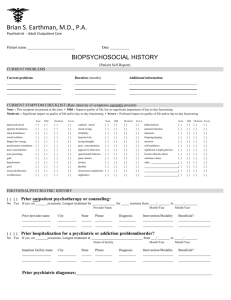
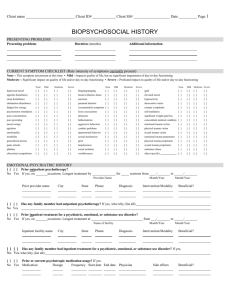
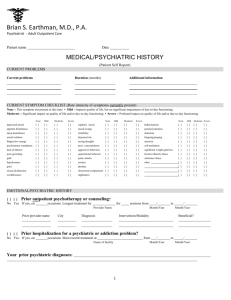
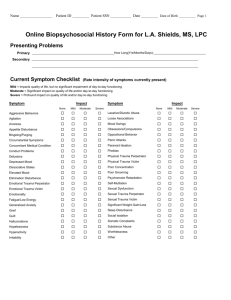
Open Arms Psychological Services 4301 Sergeant Rd. Suite 210 Sioux City, IA 51106 BIOPSYCHOSOCIAL HISTORY PRESENTING PROBLEMS What brings you in today: __________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ CURRENT SYMPTOM CHECKLIST (Rate intensity of symptoms you have had IN THE LAST 30 DAYS) None This symptom not present at this time • Mild Impacts quality of life, but no significant impairment of day-to-day functioning Moderate Significant impact on quality of life and/or day-to-day functioning • Severe Profound impact on quality of life and/or day-to-day functioning None Mild Moderate Severe None Mild Moderate Severe None Mild Moderate Severe depressed mood [ ] [ ] [ ] [ ] food bingeing/purging [ ] [ ] [ ] [ ] guilt [ ] [ ] [ ] [ ] changes in appetite [ ] [ ] [ ] [ ] nightmares [ ] [ ] [ ] [ ] elevated mood [ ] [ ] [ ] [ ] problems sleeping [ ] [ ] [ ] [ ] anorexia [ ] [ ] [ ] [ ] hyperactivity [ ] [ ] [ ] [ ] bladder/bowel problems [ ] [ ] [ ] [ ] paranoia [ ] [ ] [ ] [ ] feel like you are not part of self [ ] [ ] [ ] [ ] fatigue/low energy [ ] [ ] [ ] [ ] crying spells [ ] [ ] [ ] [ ] consistent body aches [ ] [ ] [ ] [ ] little interest in things [ ] [ ] [ ] [ ] lack of motivation [ ] [ ] [ ] [ ] self-harming behaviors [ ] [ ] [ ] [ ] poor concentration [ ] [ ] [ ] [ ] delusions [ ] [ ] [ ] [ ] significant weight gain/loss [ ] [ ] [ ] [ ] poor grooming [ ] [ ] [ ] [ ] hallucinations [ ] [ ] [ ] [ ] suicidal thoughts [ ] [ ] [ ] [ ] mood swings [ ] [ ] [ ] [ ] aggressive behaviors [ ] [ ] [ ] [ ] emotional trauma victim [ ] [ ] [ ] [ ] physical agitation [ ] [ ] [ ] [ ] conduct problems [ ] [ ] [ ] [ ] physical trauma victim [ ] [ ] [ ] [ ] emotionality [ ] [ ] [ ] [ ] helplessness [ ] [ ] [ ] [ ] sexual trauma victim [ ] [ ] [ ] [ ] irritability [ ] [ ] [ ] [ ] sexual dysfunction [ ] [ ] [ ] [ ] emotional trauma perpetrator [ ] [ ] [ ] [ ] generalized anxiety [ ] [ ] [ ] [ ] grief [ ] [ ] [ ] [ ] physical trauma perpetrator [ ] [ ] [ ] [ ] panic attacks [ ] [ ] [ ] [ ] hopelessness [ ] [ ] [ ] [ ] sexual trauma perpetrator [ ] [ ] [ ] [ ] excessive fears [ ] [ ] [ ] [ ] social isolation [ ] [ ] [ ] [ ] substance abuse [ ] [ ] [ ] [ ] compulsive behaviors [ ] [ ] [ ] [ ] worthlessness [ ] [ ] [ ] [ ] other (specify) [ ] [ ] [ ] [ ] EMOTIONAL/PSYCHIATRIC HISTORY [ ] No [ ] Yes Prior provider name [ ] No Prior or current outpatient mental health therapy? If yes, on __________________ occasions. Reason for therapy Dates of services [ ] Yes Prior hospitalizations or residential treatment for a psychiatric or mental health? If yes, on Facility name Reason for admission occasions. Dates of services [ ] No [ ] Yes Prior or current medication use FOR MENTAL HEALTH ISSUES OR SLEEP? If yes, please list past and current medications, dosages, frequency, start and stop dates, and effectiveness: [ ] No [ ] Yes Do you have ADVANCED PSYCHIATRIC DIRECTIVES IN PLACE? [ ] No [ ] Yes Has any family member received any form of mental health services including names of mental health medications? If yes, who/why (list all): Client Name: Client #: Insurance #: Open Arms Psychological Services 4301 Sergeant Rd. Suite 210 Sioux City, IA 51106 FAMILY HISTORY FAMILY OF ORIGIN Present during childhood: Present entire childhood mother [ ] father [ ] stepmother [ ] stepfather [ ] brother(s) [ ] sister(s) [ ] other (specify) [ ] Present part of childhood [ ] [ ] [ ] [ ] [ ] [ ] [ ] Age you left parent’s home: Not present at all [ ] [ ] [ ] [ ] [ ] [ ] [ ] Parents' current marital status: [ ] married to each other [ ] separated for years [ ] divorced for years [ ] mother remarried times [ ] father remarried times [ ] mother involved with someone [ ] father involved with someone [ ] mother deceased for years age of patient at mother's death [ ] father deceased for years age of patient at father's death Describe parents: Father full name occupation education general health Mother Describe childhood family experience: [ ] outstanding home environment [ ] normal home environment [ ] chaotic home environment [ ] witnessed physical/verbal/sexual abuse toward others [ ] experienced physical/verbal/sexual abuse from others Why did you leave? Special circumstances in childhood: IMMEDIATE FAMILY Marital status: [ ] single, never married [ ] engaged months [ ] married for years [ ] divorced for years [ ] separated for years [ ] divorce in process months [ ] live-in for years [ ] prior marriages (self) [ ] prior marriages (partner) Intimate relationship: [ ] never been in a serious relationship [ ] not currently in relationship [ ] currently in a serious relationship List all persons currently living in patient's household: Name Age Sex Relationship to patient Relationship satisfaction: [ ] very satisfied with relationship [ ] satisfied with relationship [ ] somewhat satisfied with relationship [ ] dissatisfied with relationship [ ] very dissatisfied with relationship List children not living in same household as patient: Frequency of visitation of above: Reason for children not living in same household: Describe any past or current significant issues in romantic relationships: Describe any past or current significant issues in other immediate family relationships: MEDICAL HISTORY (check all that apply for patient) Describe current physical health: [ ] Good [ ] Fair [ ] Poor Currently pregnant? [ ] No [ ] Yes, months along List name of primary care physician: Name Phone Practice: _____________________ City: _________________ Client Name: Client #: Is there a history of any of the following in the family: [ ] tuberculosis [ ] heart disease [ ] birth defects [ ] high blood pressure [ ] thyroid problems [ ] diabetes [ ] cancer [ ] Alzheimer's disease/dementia [ ] mental retardation [ ] stroke [ ] other chronic or serious health problems Insurance #: Open Arms Psychological Services 4301 Sergeant Rd. Suite 210 Sioux City, IA 51106 MEDICAL HISTORY Cont. (apply to patient) List past or current medical conditions, include dates of diagnosis: List any medications currently being taken for medical purpose including dosage and reason: List any known allergies, including allergies to medications: Describe any hospitalizations, accidents, or surgeries including dates: SUBSTANCE USE HISTORY (check all that apply for patient) Substances Used Complete for Lifetime Age of First Use Date of Last Use How Drug Was Used (i.e.smoked, IV, snorted, drank) How Much and How Often Was Used at Height of Use How Much and How Often Used Currently Alcohol Amphetamines/Speed Methamphetamines Barbiturates/Downers Caffeine Cocaine Hallucinogens (LSD, PCP) Inhalants Marijuana Nicotine/Cigarettes K-2 Prescriptions ABUSE Ecstasy Steroids Over the Counter Other: Family alcohol/drug abuse history: Consequences of YOUR substance abuse (check all that apply): [ [ [ [ [ [ [ [ [ [ ] father ] mother ] grandparent(s) ] sibling(s) ] other [ [ [ [ ] stepparent/live-in ] uncle(s)/aunt(s) ] significant other ] children ] hangovers ] seizures ] blackouts ] overdose ] other [ [ [ [ ] withdrawal symptoms [ ] sleep disturbance ] medical conditions [ ] assaults ] tolerance changes [ ] suicidal impulse ] loss of control amount used [ [ [ [ ] binges ] job loss ] arrests ] relationship conflicts Treatment history: List all substance abuse treatment episodes [ ] outpatient: [ ] inpatient: [ ] 12-step program meetings [ ] stopped on own [ ] other: Number of 12 step meetings in last 30 days: ____________ Client Name: Number of days of work/school missed in last 6 months due to use: ____________ Client #: Insurance #: Open Arms Psychological Services 4301 Sergeant Rd. Suite 210 Sioux City, IA 51106 DEVELOPMENTAL HISTORY (check all that apply for patient) Problems during mother's pregnancy: [ ] none [ ] high blood pressure [ ] kidney infection [ ] emotional stress [ ] bleeding [ ] alcohol use [ ] drug use [ ] cigarettes use [ ] other: ____________ _____________________ Birth: [ ] normal delivery [ ] difficult delivery [ ] cesarean delivery [ ] complications ___________________ Infancy: [ ] feeding problems [ ] sleep problems [ ] toilet training problems Delayed developmental milestones (check only those milestones that did NOT occur at expected age): [ [ [ [ [ [ [ [ [ ] sitting ] rolling over ] standing ] walking ] feeding self ] speaking words ] speaking sentences ] controlling bladder ] other Childhood health: [ ] chickenpox (age ) [ ] German measles (age ) [ ] red measles (age ) [ ] rheumatic fever (age ) [ ] whooping cough (age ) [ ] scarlet fever (age ) [ ] autism [ ] ear infections [ ] allergies to [ ] significant injuries [ ] chronic, serious health problems [ [ [ [ [ [ [ [ ] controlling bowels ] sleeping alone ] dressing self ] engaging peers ] tolerating separation ] playing cooperatively ] riding tricycle ] riding bicycle [ [ [ [ [ [ [ [ ] lead poising (age ] mumps (age ] diphtheria (age ] poliomyelitis (age ] pneumonia (age ] tuberculosis (age ] mental retardation ] asthma Emotional / behavior problems in YOUR childhood (check all that apply): [ [ [ [ [ [ [ [ [ [ ] drug use ] alcohol abuse ] chronic lying ] stealing ] violent temper ] fire-setting ] hyperactive ] animal cruelty ] assaults others ] disobedient [ [ [ [ [ [ [ [ [ [ ] repeats words of others ] not trustworthy ] hostile/angry mood ] indecisive ] immature ] bizarre behavior ] self-injurious threats ] frequently tearful ] frequently daydreams ] lack of attachment [ [ [ [ [ [ [ [ [ ] distrustful ] extreme worrier ] self-injurious acts ] impulsive ] easily distracted ] poor concentration ] often sad ] breaks things ] other Social interaction in childhood (check all that apply): Intellectual / academic functioning (check all that apply): [ [ [ [ [ [ [ [ ] normal social interaction ] isolates self ] very shy ] alienates self [ [ [ [ ) ) ) ) ) ) ] inappropriate sex play ] dominates others ] associates with acting-out peers ] other ] normal intelligence [ ] authority conflicts ] high intelligence [ ] attention problems ] learning problems [ ] underachieving ] special education during grades ______________ Current or highest education level: [ ] mild retardation [ ] moderate retardation [ ] severe retardation [ ] IEP for ___________ Field of Study: Describe any developmental problems or issues checked above: SOCIO-ECONOMIC HISTORY (check all that apply for patient) Living situation: [ ] housing adequate [ ] homeless [ ] housing overcrowded [ ] dependent on others for housing [ ] housing dangerous/deteriorating [ ] living companions actively using Social support system: [ ] supportive network [ ] few friends [ ] substance-use-based friends [ ] no friends [ ] distant from family of origin Sexual history: [ ] heterosexual orientation [ ] homosexual orientation [ ] bisexual orientation [ ] currently sexually active [ ] currently sexually satisfied Additional information: [ [ [ [ [ ] currently sexually dissatisfied ] age first sex experience ] age first pregnancy/fatherhood ] history of promiscuity age to ] history of unsafe sex age to Describe any problems with housing or support systems: Client Name: Client #: Insurance #: Open Arms Psychological Services 4301 Sergeant Rd. Suite 210 Sioux City, IA 51106 SOCIO-ECONOMIC HISTORY Cont. (check all that apply for patient) Military history: [ ] never in military [ ] served in military no combat [ ] served in military combat history Branch: _____________________ Discharge: Disciplinary Actions: Financial situation: [ ] no current financial problems [ ] large indebtedness [ ] poverty or below-poverty income [ ] impulsive spending [ ] relationship conflicts over finances Primary Source of Income: __________________________ Monthly Gross Income: _____________________________ Employment: [ ] employed fulltime-Employer: [ ] employed part-time-Employer: [ ] unemployed How long and why: [ ] history of coworker conflicts-Explain: [ ] history of supervisor conflicts-Explain: [ ] unstable work history-Explain: [ ] disabled: Longest Employment-Employer and how long: Legal history: [ ] no legal problems [ ] history of arrests List ALL arrests and dates: [ ] now on parole/probation P.O. name: [ ] history of being in jail/prison List all time served, offenses, and dates: Current length of parole/probation: [ ] any history of involvement with Child Protective Services as a child or adult List circumstances regarding involvement: Activities of daily living (check all that the patient needs assistance with to complete including reminders): [ ] none [ ] bathing [ ] personal hygiene [ ] taking medications [ ] paying bills/finances [ ] yard work [ ] shopping [ ] cooking [ ] transportation [ ] accessing community resources [ ] dressing [ ] household cleaning What assistance do you need with the above activities? Cultural/spiritual/recreational history: Cultural/religious identity (for example-ethnicity, religion): Describe any cultural issues: Currently active in community/recreational activities? YES [ ] NO [ ] Describe any hobbies: Formally active in community/recreational activities? YES [ ] NO [ ] Describe personal strengths, skills, or talents: Client Name: Client #: Insurance #: