Local Anesthetics Guide
advertisement

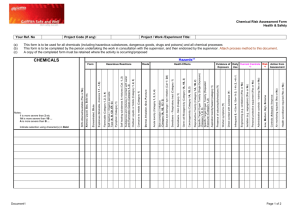
Chemical Properties of Local Anesthetics The most common local anesthetics we use for nerve blocks the the ones below. Agent Lipid Solubility Mepivacaine 1 4 Lidocaine Bupivacaine 28 Ropivacaine Not established Relative Potency Protein Binding% Duration pKa Onset Time 2 75 Medium 7.6 Quick 4 65 Medium 7.7 Quick 16 95 Long 8.1 Moderate 16 94 Long 8.1 Moderate Systemic Vascular Absorption of Local Anesthetic from Different Regional Techniques. Intercostal nerve block>Caudal>Epidural>Brachial Plexus>Sciatic-Femoral>Subcutaneous Onset Times of Local Anesthetics for Specific Peripheral Nerve Blocks Local Anesthetic Regional Block Approximate Time To Surgical Anesthesia 10 – 15mins Mepivacaine or Lidocaine 1.5% Interscalene Interscalene 15 – 20mins Ropivacaine 0.5% 15 – 30mins Mepivacaine or Lidocaine 1.5% Axillary Axillary 20 – 40mins Ropivacaine 0.5% Sciatic 30 – 45mins Ropivacaine 0.5% Femoral 15 – 20mins Ropivacaine 0.5% Maximum Doses of Local Anesthetics Local Anesthetic Dose (mg/kg) without epinephrine 5 5 3–4 2.5 Dose (mg/kg) with epinephrine 7 7 3–4 2.5 Lidocaine Mepivacaine Ropivacaine Bupivacaine Systemic Toxicity Systemic toxicity is a result of local anesthetic overdose with subsequently high serum levels. The potential for systemic toxicity is directly proportional to the intrinsic potency of the local anesthetics: Lidocaine < Mepivacaine < Ropivacaine < Bupivacaine Most toxic reactions to local anesthetics involve the central nervous system (CNS). Cardiovascular depression occurs at much higher blood levels, produces more severe consequences, and is more difficult to manage than CNS toxicity. Bupivacaine is the most cardiotoxic of all the local anesthetics agents due to its strong affinity for the cardiac calcium channel and intravascular injection of bupivacaine may result in cardiovascular collapse prior to the onset of CNS toxicity. CNS Toxicity Local anesthetics produce CNS toxicity proportional to their potency. When combining local anesthetics the potency is additive. With bupivacaine seizures occur at venous blood levels of 2 – 4mcg/mL, with lidocaine at venous blood levels of 10mcg/mL. Cardiovascular Toxicity Toxic blood levels of local anesthetics affect vessel tone, myocardial contractility, cardiac rhythm and conduction. CNS toxicity usually precedes CV toxicity however, with a drug such as bupivacaine myocardial depression can occur before CNS manifestations appear. At equipotent doses bupivacaine depresses cardiac conduction more than lidocaine. This is due to the five fold greater potency of bupivacaine as a calcium channel antagonist. Caution: Hypoxia and acidosis increase the cardiac toxicity of local anesthetics, bupivacaine in particular. Both newborns and pregnant females are more susceptible to bupivacaine toxicity. Resuscitation Algorithm for Local Anesthetic Toxicity Establish an airway and assure adequate ventilation. Administer 100% oxygen. Promptly control convulsions by administering: midazolam (2 – 5mg) or propofol (5mg increments). Establish EKG and blood pressure monitoring. Control ventricular arrhythmias with amiodarone and cardioversion (never use lidocaine). Treat myocardial depression with ephedrine or small doses of epinephrine (10 – 20mcg increments). Treat severe bradycardia or asystole with epinephrine. Bupivacaine induced asystole will require administration of large doses of epinephrine (1mg increments). For refractory malignant cardiac arrhythmias (ventricular tachycardia and fibrillation) associated with intravenous bupivacaine injection, which are unresponsive to cardioversion and amiodarone, consider emergency cardiopulmonary bypass.