Cevolution 2015T3_02_Clinical trials of antibiotics are becoming
advertisement

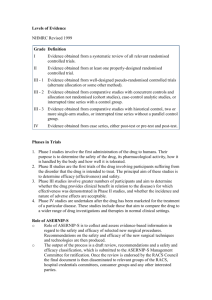
Clinical trials of antibiotics are becoming more demanding, more reliable... and (probably) less common Placebo trials. Disease indications that do not heal spontaneously without antibiotics. Field trials that have a closer resemblance to the conditions of use in the field. Second choice antibiotics that are actually tested as second intention... The new guideline on the efficacy of new antibiotics toughens the requirements, with the risk of discouraging their development. The European Medicines Agency (EMA) has published a draft of new guidelines on the demonstration of efficacy of veterinary antibiotics. The objective is clear. For antibiotics to be used less and better, they should also be assessed better. However, there will probably also be less candidate substances submitted for assessment. The highlights of the future guideline include the following points. Metaphylaxis and antibiotic prevention: against placebo This is new: the guideline recognises the possibility to claim an efficacy for metaphylactic use, but only in addition to a curative efficacy in diseased animals – because metaphylaxis is defined as the treatment of apparently healthy animals that are in contact with diseased animals (treated curatively). Nor does the guideline exclude indications for prevention in case of high and severe infectious risk. However, the trials demonstrating efficacy for metaphylactic or preventive treatment will need to be compared to placebo treatment, and on good farms where antibiotics are not used to mask poor hygiene. Such trials will be difficult to set up. For oral treatment of animals in groups (oral powders and drinkable solutions), the metaphylactic indication may be demonstrated on the basis of (tangible) results of the curative treatment trial of groups including both healthy and diseased animals. That may be easier to prove for oral substances than for injectables. Placebo to assess spontaneous recovery Until now, clinical trials have been comparative trials, mainly with older reference antibiotics. The benefits compared to a spontaneous recovery (placebo) or non-antibiotic measures were therefore not evaluated. The new guideline recommends trials against placebo, even if the spontaneous recovery rate is high, in particular in case of benign and transitory infections or multifactorial diseases. The benefits of antibiotic therapy over other, non-antibiotic measures should be clearly demonstrated. Certain indications listed in the data sheet may no longer be acceptable in future. Field trials closer connected to the field Currently, field trials often lead to an overestimation of antibiotic efficacy compared to the usual field conditions, due to the inclusion criteria and the exclusion of severe, recurring or chronic cases (which are the most difficult to treat). In future, the target animals should closer resemble those found in the field. Clinical trials should be more realistic. The objective is no longer limited to the demonstration of efficacy by selecting cases that are likely to respond well to antibiotics, but also to better assess the recovery rates in the field. A ‘good’ reference treatment In comparative trials, the choice of the reference treatment is essential. The equivalence or superiority of a new antibiotic will be easier to prove if compared to a moderately efficacious antibiotic. The guideline demands that the efficacy of the reference antibiotic (at the approved dose) is validated using recent sensitivity data. In other words, it will no longer be possible to compare with a “poor” antibiotic, even if it is approved for the target indication. 2nd intention trials for 2nd intention antibiotics Clinical trials should follow the official recommendations of antibiotic classification (1st or 2nd intention) in particular concerning critical antibiotics: third and fourth generation cephalosporins and fluoroquinolones. The clinical trials of these last-resort antibiotics should therefore be organised to include (expected) therapeutic failure. However, to take into account the difficulty of organising such trials in a large number of animals, the trials performed for second intention could be carried out in a limited number of animals (without conclusive statistical results), in addition to a trial demonstrating first-line efficacy (with conclusive statistical results). A preference for plasma concentrations … The pharmacokinetics/pharmacodynamics (PK/PD) approach, which consists of comparing the in vivo concentration to the in vitro MIC, is well known. The new guidelines prefer this approach in order to confirm a therapeutic dose or even to confirm an efficacy for rare indications, including infections due to multiresistant bacteria. The study is preferably carried out on the free fraction of the plasma concentration, as this corresponds well to the levels in the biophase, where extracellular germs multiply. The approach using tissue concentrations will need to be validated on forehand, which means it is probably avoided. However, it seems to be accepted that this approach is not valid for all antibiotics. Macrolides in particular have very low plasma concentrations, well below the MIC. Finally the MIC data must be recent (less than 5 years old). “As short as possible” The guideline encourages performing population pharmacokinetic studies on the basis of field trials (among others for oral powders and oral solutions). The duration of exposure to antibiotics, which cannot be determined by a PK/PD approach, should be “as short as possible”. The objective is the avoidance of “unnecessary exposure to antibiotics” and that of “unnecessary selection pressure of resistant bacteria”. Clinical and bacteriological recovery The efficacy should be assessed within a period to be justified, based on clinical, and if possible, bacteriological criteria. This supposes sampling animals that appear healthy at the end of the study. The clinical response is generally the first criterion of efficacy (with exceptions). In group treatment, e.g. in poultry, where individual assessment is not possible, the efficacy is assessed for the group (e.g. evolution of the mortality rate) and based on post-mortem examination with bacteriological analysis. The guideline also demands a post-treatment follow-up to assess any possible relapses (due to an insufficient efficacy) by separating them from relapses due to a re-infection (possibly by another germ). If possible, bacteriological test should be carried out in case of treatment failure and relapses. Source: European Medicines Agency (EMA). Second consultation of the guideline for the demonstration of efficacy for veterinary medicinal products containing antimicrobial substances. Reference document EMA/CVMP/261180/2012.