MRI Patient Screening
advertisement

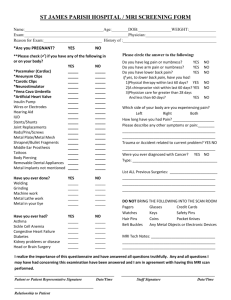
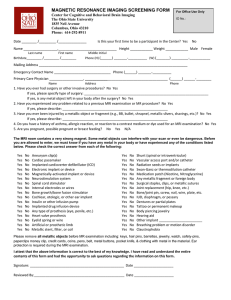
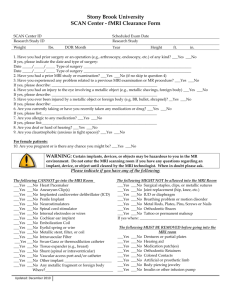
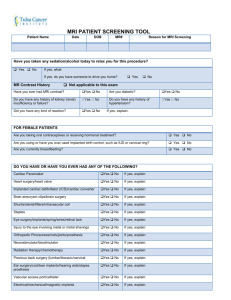
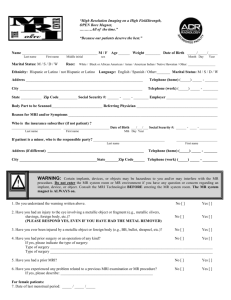
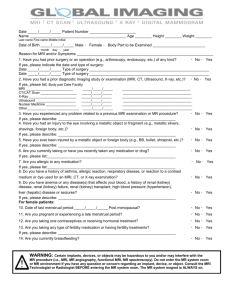
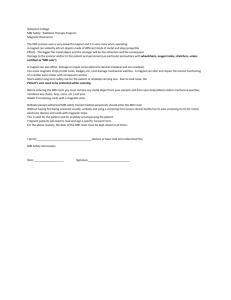
MRI SCREENING FORM Name:_________________________________________________ Birth Date:_____/_____/_____ Height:____________________ Weight:___________________ Diabetic or kidney problems? NO YES Have you ever had surgery? NO YES If yes please list: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Have you ever had an eye injury involving metal? (Grinding, fabrication, etc.) NO YES If yes please describe:___________________________________________________________________ Are you pregnant and/or breastfeeding? NO YES WARNING: Some of the following items may be extremely hazardous to your safety and interfere with the MRI exam. Please circle YES or NO if you have following. NO YES Cardiac pacemaker NOtheYES Shrapnel, buckshot, or bullets NO NO NO NO NO NO NO NO NO NO NO NO NO NO YES YES YES YES YES YES YES YES YES YES YES YES YES YES NO YES NO YES NO YES NO YES Implanted Cardiac Pacemaker / Defibrillator Aneurysm clip or brain clip Carotid artery vascular clamp Neurostimulator Insulin or Infusion pump Claustrophobia Spinal Fusion Stimulator Cochlear Implant or Ear tubes Prosthesis (eye, penile, etc.) Magnetic Implant (dental, etc.) Heart Valve replacement Artificial limb or joint Electrodes (on body, head or brain) Intravascular stents, filters or coils Shunt (spinal or intraventricular) Ports or catheters Transdermal medicine patches (smoking, pain, etc.) Hearing Aids NO NO NO NO NO NO NO NO NO NO NO NO NO NO YES YES YES YES YES YES YES YES YES YES YES YES YES YES IUD, Diaphragm Pessary or bladder ring Tattooed eye liner or eyebrows Body piercings Metal Fragments Cosmetic Surgery Internal pacing wires Aortic Clips Venous Umbrella Metal or wire mesh Wire sutures or staples Harrington rods Screws, pins or nails in the bone Wig, toupee or hair implants NO YES Dentures (remove before scan) NO YES Asthma or breathing disorder NO YES Seizures or motion disorders IMPORTANT INSTRUCTIONS: Remove all metallic objects before entering MRI including hearing aids, cell phone, keys, glasses, hair pins/barrettes, jewelry, watch, safety pins, money clips, credit/bank cards, and coins. Loose metallic objects are especially prohibited in the MRI environment. Please consult the MRI Technologist if you have any questions or concerns BEFORE your scan. Patient/Legal Guardian Signature:___________________________________ Date: _____/_____/_____ MRI Technologist Signature:_______________________________________