Epinephrine administration request
advertisement

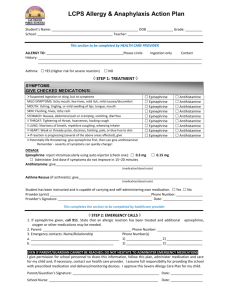
File: JHCD-E LEXINGTON CITY PUBLIC SCHOOLS 300 DIAMOND STREET, LEXINGTON, VIRGINIA 24450 Name of School: __________________________________ School Year: ___________________ MEDICATION PERMISSSION FORM - PRESCRIBED EPINEPHRINE – CONSENT FOR ADMINISTRATION Student Name: _____________________________________________________________________________ PRESCRIBING PHYSICIAN: This student may have a severe allergic reaction to I have attached the required Food Allergy Action Plan which describes this student’s potential symptoms. Yes No Any SEVERE SYMPTOMS after suspected or known contact with allergen: One or more of the following: 1. Heart rate greater than 120 times a minute, systolic blood pressure less than 80. 2. Breathing rate less than 12 or greater than 36 times a minute. 3. Significant wheezing or poor air movement. 4. Overwhelming generalized hives or sudden onset of swelling. 5. An anxious student or a student with decreased consciousness. 6. Drooling, hoarse voice, and/or inability to swallow. 1. INJECT EPINEPHRINE IMMEDIATELY 2. Call 911 3. Begin monitoring student: Stay with student, have parent notified, continuing symptoms, what time was epinephrine given 4. Give additional medications: - Antihistamine - Inhaler if asthmatic MILD SYMTPOMS: 1. Few hives, mild itch 2. Mild nausea/discomfort 1. GIVE ANTIHISTAMINE 2. Stay with student; alert parent 3. If symptoms progress as above USE EPINEPHRINE 4. Begin monitoring as above It is necessary for him/her to carry an Epi-Pen with them during the school day, during activities, and in transit to and from school. Yes No The student knows how to use the injectable and has demonstrated the ability to administer Yes No Medications Prescribed: Epinephrine ___________________________________________________________________ Antihistamine _________________________________________________________________ Other (e.g., inhaler) _____________________________________________________________ _____________________________________________________ Physician Signature PARENT: _______________________________________ Date I am in agreement with this plan of care, and I give permission for the school to follow this. I understand that the principal may rescind this privilege if my child fails to handle the medication safely and appropriately. Epi-Pen to be kept with student Epi-Pen to be kept in office Epi-Pen to be kept with teacher Parent/Guardian Signature LEXINGTON CITY PUBLIC SCHOOLS Date