Glioma stem cells
advertisement

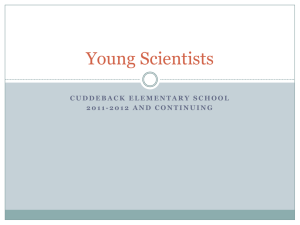
Glioma stem cells Evidence supporting the cancer stem cell hypothesis for gliomas and technical approaches to investigate glioma stem cells Marloes van den Nieuwendijk Writing assignment Neuroscience and Cognition | Experimental and Clinical Neuroscience track Student number 3501981 Supervised by professor dr. E.M. Hol March 2014 PREFACE This writing assignment for the master Neuroscience and Cognition is the result of five weeks of intensive literature search about glioma stem cells and their capacity to form and propagate gliomas. The first chapter of this writing assignment provides an overview of the characteristics of gliomas. A detailed overview the characteristics of glioma stem cells is provided in the second chapter. Here, also the possible cell types from which glioma stem cells might arise are summarized. The evidence supporting the view that gliomas arise from glioma stem cells is summarized in chapter three and the available in vitro and in vivo models for glioma stem cell research are addressed in chapter four. Finally, the remaining questions concerning the cell of origin of gliomas are identified in the fifth chapter. I would like to thank prof. dr. E.M. Hol for her enthusiasm for the subject and the instructive feedback. 2 ABSTRACT Gliomas are the most common primary brain tumors and especially high grade gliomas have a bad prognosis. Treatment comprises surgery, radiotherapy and chemotherapy, but this approach often fails because tumor cells become resistant to therapy and it is extremely difficult to remove all tumor cells. Understanding the cell of origin of gliomas might be the only way to develop more effective treatment strategies. The main hypothesis concerning the glioma cell of origin is that gliomas arise from glioma stem cells, which are capable of self-renewal and generate a heterogeneous tumor containing both stem cells and cells which lack the capacity to self-renew. It remains unclear if neural stem cells give rise to glioma stem cells or whether glioma stem cells derive from committed neural progenitors or from differentiated neurons or astrocytes. The main questions that is discussed in this writing assignment is which recent experimental findings are in line with the hypothesis that gliomas arise from glioma stem cells. Furthermore, the question which in vitro and in vivo techniques can be used to study glioma stem cells will be addressed. Finally, the remaining questions in the field of glioma stem cell research are discussed. LAYMEN ABSTRACT Gliomas are brain tumors which contain glial cells. Glial cells have several functions in the brain, including providing support to brain cells. In the Netherlands, about 1000 people are diagnosed with glioma every year. Glioma symptoms include headache, memory problems, personality changes and seizures and have a strong impact on the patients’ life. The majority of glioma patients suffers from an incurable form. Patients diagnosed with the most aggressive form survive on average for 10 months after diagnosis. It is thought that the formation of gliomas might be caused by stem cells. Stem cells are capable of self-renewal, which means that they can divide and thereby form new stem cells and other cells, which are not stem cells. A second important feature of stem cells is that they can divide into different cell types. It is thought that the formation of gliomas is caused by specific, mutated stem cells, which are called glioma stem cells. These cells comprise only a small part of the tumor, but they can make a tumor mass by high levels of cell division. Over time they acquire more mutations and can for example become resistant to chemotherapy and radiotherapy. The current glioma treatment, which can only extend the patients’ life with a couple of months, tries to destroy the entire tumor. The identification of glioma stem cells indicates that new treatment should be targeting the glioma stem cells, because if they remain present in the brain after therapy, the tumor will regrow. However, there are still a lot of questions about the existence and characteristics of glioma stem cells. Thus, to develop better treatment options for gliomas, it is crucial to understand the characteristics of glioma stem cells and know how gliomas are formed. The main question which is addressed in this writing assignment is what evidence supports the idea that glioma stem cells can cause the formation of gliomas. Furthermore, the question how glioma stem cells can be studied will be discussed. Finally, the remaining questions in the field of glioma research will be discussed. 3 ABBREVIATIONS Ara-C BBB BrdU CD15 CD133 Cnp CSC DG DNA EGF EGFR FGF GCL GFAP GFP GIC GSC LGR5 LIF MAP2 MGMT miR-200c NOD-SCID NSC OPC PC PCR PDGF-B SGL shRNA Ssh SVZ WHO ZEB1 cytosine-β-D-arabinofuranoside blood-brain barrier bromodeoxyuridine cluster of differentiation-15 cluster of differentiation-133 2’,3’-cyclic nucleotide 3’-phosphodiesterase cancer stem cell dentate gyrus deoxyribonucleic acid epidermal growth factor epidermal growth factor receptor fibroblast growth factor granule cell layer glial fibrillary acidic protein green fluorescent protein glioma initiating cell glioma stem cell leucine-rich repeat containing G protein-coupled receptor 5 leukemia inhibitory factor microtubule associated protein 2 O6-methylguanine DNA methyltransferase micro ribonucleic acid-200c non-obese diabetic, severe combined immunodeficient neural stem cell oligodendrocyte precursor cell progenitor cell polymerase chain reaction platelet-derived growth factor B subgranular layer short hairpin ribonucleic acid sonic hedgehog subventricular zone World Health Organization zinc finger E-box binding homeobox 1 4 INDEX Preface................................................................................................................................................. 2 Abstract ............................................................................................................................................... 3 Laymen abstract .................................................................................................................................. 3 Abbreviations ...................................................................................................................................... 4 Index .................................................................................................................................................... 5 1. Gliomas ............................................................................................................................................ 6 2. The cancer stem cell hypothesis for gliomas .................................................................................. 8 2.1 The cancer stem cell hypothesis ............................................................................................... 8 2.2 Glioma stem cells..................................................................................................................... 10 2.3 Cell of origin of glioma stem cells ............................................................................................ 11 3. Evidence supporting the hypothesis that gliomas arise from glioma stem cells .......................... 14 4. Research techniques to investigate glioma stem cells .................................................................. 16 4.1 In vitro models for human gliomas.......................................................................................... 16 4.2 In vivo models for human gliomas........................................................................................... 17 5. Remaining questions and conclusion ............................................................................................ 18 References ......................................................................................................................................... 20 5 1. GLIOMAS Gliomas, which are highly heterogeneous brain tumors composed of glial cells, are the most common primary brain tumors. They are categorized according to the type of glial cell found in the tumor. These categories are astrocytomas, which contain astrocytes, oligodendrogliomas, which consist of oligodendrocytes, and ependymomas, which contain ependymal cells1. Mixed tumors consisting of both astrocytes and oligodendrocytes, which are called oligoastrocytomas, or tumors containing both glial cells and neurons, including gangliogliomas and gangliocytomas, are also known2. In the Netherlands, the glioma incidence remains stable with an incidence of 4 or 6 per 100.000 personyears for females and males respectively3. Astrocytomas are the most common glial tumors, with an average incidence of 4.8 cases per 100.000 people per year in Europe4. The majority of the astrocytoma patients suffers from glioblastoma5. Oligodendrogliomas and ependymomas have a lower incidence, with 0.4 and 0.2 cases per 100.000 people per year 4. Based on histopathological characteristics which can be observed with light microscopy, gliomas are divided into four grades in the classification of the World Health Organization (WHO) (Table 1). The WHO grade predicts the biological behavior of the tumor and subsequently relates to the preferred treatment options and clinical outcome. WHO grades I and II are considered benign gliomas, while grades III and IV are malignant gliomas2. Since astrocytomas have the highest incidence of all gliomas4, the histological abnormalities found in these tumors are summarized here. Grade I pilocytic astrocytomas show low levels of proliferation and contain bipolar cells which have dense glial fibrillary acidic protein (GFAP) positive protrusions. Astrocytomas containing GFAP meshworks and cells with aberrant nuclei are classified as grade II astrocytomas, including diffuse astrocytomas. Grade III anaplastic astrocytomas show aberrant nuclei, high levels of mitotic activity and anaplasia. Grade IV glioblastomas also show necrosis and/or microvascular proliferation, next to aberrant nuclei, high levels of mitotic activity and anaplasia1,2. Table 1. WHO classification of gliomas. Names of tumors (left column) are followed by the cell type(s) which are found in the tumor (middle column) and the WHO grade (right column). Adapted from Louis et al. 2007 Tumor: Subependymal giant cell astrocytoma Pilocytic astrocytoma Pilomyxoid astrocytoma Diffuse astrocytoma Pleomorphic xanthoastrocytoma Anaplastic astrocytoma Glioblastoma Giant cell glioblastoma Gliosarcoma Oligodendroglioma Anaplastic oligodendroglioma Oligoastrocytoma Cell type(s) of tumor: Astrocytes Astrocytes Astrocytes Astrocytes Astrocytes Astrocytes Astrocytes Astrocytes Astrocytes WHO grade: I I II II II III IV IV IV Oligodendrocytes Oligodendrocytes II III Astrocytes and oligodendrocytes II 6 Anaplastic oligoastrocytoma Astrocytes and oligodendrocytes III Subependymoma Myxopapillary ependymoma Ependymoma Anaplastic ependymoma Ependymal cells Ependymal cells Ependymal cells Ependymal cells I I II III However, the microscopic abnormalities observed in biopsy samples only provide information about a small part of the glioma. Because of the heterogeneous nature of gliomas, grading based on biopsy samples is frequently not correct when compared to the surgically resected tumor and as a consequence patients do not receive optimal treatment and get a wrong prognosis6. Currently, it is becoming clear that molecular subtyping of gliomas might be a more powerful system to grade these tumors and to determine how they should be treated. With this approach, it is possible to distinguish different patients groups based on molecular markers even within a group of patients with identical histopathological classification. Thereby it can be assessed for individual patients which treatment they should receive7. O6-methylguanine DNA methyltransferase (MGMT) promoter methylation is one of the identified molecular markers for gliomas. The MGMT protein is involved in deoxyribonucleic acid (DNA) repair by removing alkylgroups from the DNA. Hypermethylation of the MGMT promoter causes silencing of the MGMT gene and thereby inhibits the removal of alkylgroups. As a consequence, the glioma cells are more sensitive to DNA damage induced by alkylating agents such as temozolomide. Thus, MGMT promoter methylation status, which can be assessed with methylation-specific polymerase chain reaction (PCR), can be used as a marker to predict the response to alkylating chemotherapy in primary gliomas8. The MGMT promoter methylation status is homogeneous throughout the glioma and thus a single biopsy sample is sufficient to determine if a patients would benefit from additional therapy with alkylating agents9. On a macroscopic level, grade I gliomas are frequently not infiltrative, whereas grade II, III and IV gliomas often infiltrate surrounding tissue. Chances of recurrence for grade II gliomas are high and a subset of grade II gliomas transforms into higher grade gliomas. Grade IV gliomas are characterized by possible metastases. Pre- and postoperative disease progression is fast and grade IV gliomas are often fatal2. Glial tumors in the CNS and pineal gland have a lower average five-year survival rate than non-glial tumors in the CNS and pineal gland. Highest five-year survival is seen in ependymoma patients, with an average of 74%, followed by oligodendroglioma patients with 55%. Five-year survival of astrocytoma patients is not more than 15%, because of the high incidence of the aggressive grade IV glioblastoma4. Glioblastoma patients have an average survival of 10 months after diagnosis. Treatment extends survival to an average of 16 months10. Standard treatment for malignant gliomas is a multimodal approach combining surgical resection, radiotherapy and chemotherapy. Nevertheless, this approach only extends survival with several months because of several complicating factors. Surgical resection of the entire tumor is complicated by the location and the invasive nature of gliomas, and thus often not all tumor cells are removed11. Furthermore, glioma cells can become resistant against radiotherapy by activating DNA repair mechanisms which thereby block the effect of radiotherapy12. A third complicating factor is the blood-brain barrier (BBB), which prevents most systemic chemotherapeutic agents from entering the glioma11. A promising approach to target gliomas is by using viruses. The idea of using of viruses in treatment of brain tumors is not new, however this method still needs to be improved. Two different 7 approaches are investigated for their use in glioma treatment. The first are the viral vectors which are used to deliver specific genes with anti-tumor activity to the glioma cells. Secondly, research focuses on the application of oncolytic viruses, which specifically infect and destroy glioma cells13. Despite the effort in improving current therapies, it is generally believed that a specific therapy for gliomas can only be developed when the cells from which gliomas originate are identified14 so that these cells can be specifically targeted. The cell type which is held responsible for glioma formation and survival, which is the glioma stem cell, is discussed in the next chapter. 2. THE CANCER STEM CELL HYPOTHESIS FOR GLIOMAS 2.1 THE CANCER STEM CELL HYPOTHESIS According to the cancer stem cell hypothesis, cancer cells in general are hierarchically organized and only a small subpopulation of cancer cells, the cancer stem cells (CSCs), is mitotically active for an indefinite period of time and has the ability to self-renew. Thereby, CSC maintain and expand the stem cell population and give rise to a heterogeneous population of cancer cells in which the remaining majority of cancer cells is not capable of self-renewal and has limited dividing potential (Fig. 1A)15,16. An evolutional view of the cancer stem cell hypothesis is that, as a consequence of natural selection and genomic instability, the hierarchy of tumor cells changes over time and new clones with different mutations appear. Eventually, the majority of these cells will have selfrenewing potential independent of their niche (Fig. 1B)17. The question is if the cancer stem cell hypothesis also applies to gliomas. The term CSC is used for cancer in general, whereas the CSCs in gliomas are called glioma stem cells (GSCs). Thus, GSCs are also characterized by their Fig 1. Overview of the classical and evolutional view of the cancer capacity for self-renewal and the stem cell hypothesis. (A) Classical view in which only the CSCs are ability to create a capable of maintaining and expanding the stem cell population and heterogeneous tumor of which differentiation into multiple cell types. (B) Evolutional view proposing the majority of cells is not that the hierarchy inside a tumor changes and causes stem cells with 18 new mutations to appear. Adapted from Chen et al, 2012. capable of self-renewal . GSCs are often confused with glioma initiating cells (GICs). As described above, GSCs are characterized by the capacity for self-renewal and the potential to give rise to heterogeneous progeny including both stem cells and cells without stem-like properties. GSCs are tumorigenic and can initiate the formation of a recurrent glioma. However, GSCs are not necessarily the cells that initiate the formation of a primary glioma. The cells that initiate the formation of gliomas, which are called GICs, are the cells that undergo the initial tumorigenic transformation and thereby give rise to a glioma containing a GSC population19. If the cancer stem cell hypothesis applies to gliomas, GSCs might arise from three possible GICs which are the adult neural stem cells (NSCs), restricted 8 progenitor cells (PCs) or mature neural cells16,20,21. NSCs might transform into GSCs by acquiring cancerous mutations which enable them to survive and self-renew in a different niche, to proliferate in the absence of a niche, to make the cells in the niche proliferate to expand the niche for the mutant stem cells, or possibly to differentiate but maintain the capacity for proliferation and reacquire the capacity for self-renewal. Also the niche itself might change and thereby allow only the survival of stem cells with specific mutations that can later make the cells cancerous16. Mechanisms which are involved in self-renewal are already activated in NSCs, thus it is hypothesized that less steps, and thus less mutations, are required for these cells to become GSCs than for mature, fully differentiated neural cells. A second reason why NSCs might be the target for cancerous transformation is that stem cells are capable of self-renewal over a long time, whereas most mature cells have a short lifespan. This makes NSCs more prone to acquire multiple mutations15. However, another possibility is that GSCs derive from restricted PCs which acquire the capacity for selfrenewal, which is a hallmark of stem cells, and become immortal through mutations16. A third possible cell of origin of GSCs are mature neural cells which acquire mutations and thereby dedifferentiate into a more stem-like cell capable of long-term self-renewal22. It is suggested that mature neural cells need more mutations than NSCs to activate the self-renewal mechanisms15. The main opposite view of the cancer stem cell hypothesis is the clonal evolution model, which implies that a tumor initially consists of equivalent tumor cells of which the majority has self-renewal capacities (Fig. 2). Over time, genetic and epigenetic events will change these cells and the clones with advantageous mutations will rule out other clones, thus selecting for clones with advantageous genetic alterations. These mutations will also cause the heterogeneity which is observed in many cancers. This model shares the feature of selection with the evolutional view of the cancer stem cell hypothesis17,20. Fig. 2. Schematic overview of the clonal evolution model, which proposes that cancer arises from equivalent cells of which most of them have the potential for self-renewal and over time cells which gain beneficial mutations will exclude other tumor cells. Adapted from Chen et al. 2012. 9 2.2 GLIOMA STEM CELLS GSCs have acquired multiple mutations over time which make them behave differently compared to NSCs, for example that GSCs proliferate with a much higher speed than NSCs23. An overview over the events required for transformation into GSCs is beyond the scope of this writing assignment. This section focuses on the most important features of GSCs. The key properties of NSCs are the capacity for self-renewal and multipotency and transformed GSCs were initially ascribed the same key properties as NSCs. Although GSCs share the capacity for self-renew with NSCs, recent evidence makes clear that GSCs should not be considered as multipotent cells. GSCs have the ability to differentiate into neurons, astrocytes or oligodendrocytes in vitro24, but the differentiated progeny has an aberrant genetic profile22. The definition now used is that GSCs can self-renew and thereby generate a heterogeneous tumor mass16. When cultured under serum- and matrix free conditions supplemented with epidermal growth factor (EGF) and fibroblast growth factor (FGF), GSCs grow in clusters of cells which are called neurospheres25. This is also characteristic of NSCs26. GSC neurospheres derived from human gliomas express proteins which are typically found in normal NSCs, such as the cytoskeletal intermediate filament nestin, the stem cell marker cluster of differentiation-133 (CD133), the RNA-binding protein musashi-1 and the transcription factor Sox212,25,27. After addition of leukemia inhibitory factor (LIF) to the medium, cultured human GSCs can differentiate into neurons, astrocytes or oligodendrocytes, which also occurs when NSCs are cultured under these conditions24. GSCs represent a minority of the total number of tumor cells in a glioma. Of great significance was the finding that the CD133 expressing tumor cells, which have the capacity for proliferation, selfrenewal and multipotency and thus display the typical stem cell properties, are crucial for formation and propagation of the tumor in vitro and in vivo, whereas CD133 negative tumor cells lack this potential. These results support the view that CD133 expressing cells are glioma stem cells18,27. When cells from human glioblastomas are dissociated into single-cell suspensions and the CD133 positive fraction is purified and injected into the frontal lobe of non-obese diabetic severe combined immunodeficient (NOD-SCID) mice, the CD133 positive cells form a tumor. Injection of 100 CD133 positive glioblastoma cells is sufficient to induce tumor formation, whereas a 500- to 1000-fold higher number of CD133 negative cells does not induce tumor formation. Tumors formed in the NOD-SCID mice display the same histological characteristics as the human glioblastoma from which they derive, such as high levels of proliferation, heterogeneous staining for nestin, expression of the astrocytic marker GFAP and the neuronal marker microtubule associated protein 2 (MAP2). CD133 positive and negative tumor cells display the same chromosomal abnormalities, which demonstrates that these cells are presumably derived from each other. Serial transplantation of CD133 expressing cells causes the formation of new tumors with similar characteristics as the original human tumor, thus indicating the self-renewing potential and the potential to propagate gliomas of CD133 positive cells in vivo. This study identifies CD133 positive cells with stem cell properties to be the causal for glioma formation and propagation18. These data are supported by a study in which cells derived from human glioblastomas are cultured in clonal density in a serum-free system with EGF and FGF2, so that differentiated cells will disappear and only GSCs remain. These GSCs are capable of tumor formation and propagation, even after serial transplantation24. 10 After receiving surgery and radiotherapy, malignant gliomas often recur and this happens almost without exception within a small margin from where the primary tumor was located. Thus, tumor regrowth occurs in the area which receives the highest dose of radiotherapy28. This suggests that a small group of cells, which is now thought to be the GSCs, is resistant to radiotherapy and is able to initiate and propagate the formation of a new tumor. This is supported by a study indicating that, following ionizing radiation exposure, the number of CD133 positive cells in cultures increases four times compared to non-irradiated cultures. In vivo, the number of CD133 positive cells present in a glioma xenograft increases three to five times after irradiation. The CD133 negative cells remain CD133 negative after receiving radiotherapy. Cultures with CD133 positive cells show a lower number of apoptotic cells compared to CD133 negative cells and nude mice transplanted with a higher percentage of CD133 positive cells of the total number of tumor cells develop tumors earlier and the tumors show increased growth and vascularization. Tumors also develop faster when tumor cells from irradiated xenografts are transplanted into the brains of other mice compared to transplantation of non-irradiated tumor cells. These data indicate that CD133 positive cells are the cause of radioresistance. CD133 positive cells derived from human glioblastomas or from xenografts are more resistant to therapy because of increased phosphorylation of checkpoint proteins which respond DNA damage. This leads to activation of these proteins, which causes cell cycle arrest, eventually leads to increased activation of DNA repair mechanisms and thereby the cell death which would be the result of radiotherapy is evaded12. 2.3 CELL OF ORIGIN OF GLIOMA STEM CELLS As discussed in the introduction of this chapter, GSCs potentially derive from three cell types: NSC, restricted PCs or mature neural cells. This section gives an overview of the most important hallmarks of these cell types and evidence that these cells can give rise to gliomas (Fig. 3). Fig. 3. An overview of the potential cell types from which GSCs might derive and the markers that are expressed by these cells. From Chen et al. 2012. NSCs are characterized by their multipotency and long-term self-renewing potential, which thereby enables them to maintain and expand the stem cell pool and to give rise to heterogeneous progeny. 11 A balance in self-renewal and differentiation is important to maintain the stem cell population and is sustained by the niche, which provides NSCs with growth factors, blood vessels and a matrix29. However it appears to be very difficult to distinguish NSCs and PCs, which hampers the investigation of the cell of origin of glioma stem cells30. In the adult human and rodent brain, the main NSC niches are the subventricular zone (SVZ) close to the lateral ventricles and the subgranular layer (SGL) of the hippocampal dentate gyrus (DG) (Fig. 4)31–34. Fig. 4 Overview of the main stem cell niches, the SGL and the SVZ, in a schematic saggital section of the adult mouse brain. The SGL and SVZ are indicated by the red boxes. SGL; subgranular layer, SVZ; subventricular zone. Adapted from Uchida et al. 2000. The murine SVZ comprises a layer of dividing cells along the lateral edge of the lateral ventricles and contains four cell types: type A neuroblasts, type B astrocytes, type C transit amplifying progenitor cells and ependymal cells. The ependymal cells separate the SVZ from the lateral ventricles. After treatment with the antimitotic agent cytosine-β-D-arabinofuranoside (Ara-C), all neuroblasts and transit amplifying cells are destroyed and start to reappear a few days after treatment. Together with the findings that all remaining cells immediately after Ara-C treatment express GFAP and that these cells incorporate a marker for DNA synthesis, these data demonstrate that type B astrocytes are the only self-renewing cells in the SVZ and thus can be seen as NSCs. Type B astrocytes divide and give rise to new stem cells and type C transit amplifying progenitors, which in turn proliferate several times and generate type A neuroblasts. The neuroblasts migrate via the rostral migratory stream into the olfactory bulb where they become interneurons. This process occurs under normal conditions32. A subset of the SVZ astrocytes has the potential to differentiate into oligodendrocyte precursor cells (OPCs) and mature oligodendrocytes in vitro and in vivo35. The human SVZ also comprises a cell population with stem cell properties31,33, but the organization of the human SVZ is different than the rodent SVZ. It comprises four layers of which the first layer is a layer of ependymal cells, followed by a hypocellular layer which contains very few cell bodies and is mainly occupied by dense astrocyteand ependymal cell protrusions. The third layer is formed by a ribbon of astrocyte cell bodies of which a subgroup is mitotically active, followed by the fourth layer of brain parenchyma which is called the transitional zone36. The astrocytes in layer three are capable of forming neurospheres and generating cells of the neuronal, astrocytic and oligodendrocytic lineage in vitro33,37. 12 A process similar to that in the SVZ occurs in the adult hippocampus. In the SGL of the mouse hippocampal DG, GFAP expressing astrocytes are found which have the same characteristics as type B astrocytes in the SVZ. These SGL astrocytes divide and thereby generate GFAP-negative type D cells and sustain the SGL stem cell pool. Type D cells in turn differentiate into new granule neurons which will be part of the DG granule cell layer (GCL)34. This is also found in postmortem brain samples from the hippocampus of patients who were treated with bromodeoxyuridine (BrdU), a marker which is incorporated into the DNA during DNA synthesis and thus labels proliferating cells. In these samples, BrdU labeled new granule cell neurons are detected in the GCL of dentate gyrus31. Evidence that NSCs can give rise to glial tumors comes for example from a mouse model in which the tumor suppressor genes pten, p53 and nf1 are exclusively inactivated in NSCs and PCs. In this model, a transgene expressing cre recombinase-modified estrogen receptor ligand-binding domain fusion protein is placed under the control of the nestin promoter. This promoter causes inactivation of the tumor suppressor genes only in NSCs and PCs. After administration of tamoxifen, the fusion protein translocates to the nucleus and recombines the tumor suppressor genes pten, p53 and nf1. All of these transgenic mice develop grade III or IV astrocytomas, which suggests that deletion of pten, p53 and nf1 restricted to NSCs and PCs is sufficient to induce astrocytomas. The labeling of NSCs and PCs with LacZ allows tracing of these cells, which reveals that NSCs and PCs from the SVZ and SGL transform into GSCs, migrate away and infiltrate surrounding tissue where they form astrocytomas. These GSCs express neuronal, astrocytic or oligodendroglial markers and thus show some level of differentiation, which might explain the heterogeneity seen in human astrocytomas. Inactivation of pten, p53 and nf1 in NSCs and their progenitors from the SVZ reveals astrocytoma formation in many brain regions, while inactivation of these tumor suppressors in regions without NSCs do not cause astrocytoma formation. Thus, NSCs and PCs are capable of initiating astrocytoma formation, whereas mature cells cannot initiate the formation of astrocytomas. The mutant SVZ NSCs or PCs show, when cultured as neurospheres, increased proliferation and diminished apoptosis38. Evidence for gliomas arising from PCs in the adult brain is also available. In a mouse model, an activated allele of the epidermal growth factor receptor (EGFR) is placed under the S100β promoter to specifically target OPCs which lost the stem cell phenotype. When this is combined with p53 deficiency, oligodendrogliomas develop in white matter regions. In the corpus callosum of these transgenic mice, three times higher numbers of OPCs are present compared to control animals, which are identified by S100β, olig2 and NG2 expression. In this mouse model, tumors arise in white matter regions and NG2 positive cells from these tumors show similar protein expression patterns compared to normal OPCs and human oligodendroglioma cells. Moreover, the expression of sox10, which is involved in OPC differentiation and the formation of gliomas, is increased in these NG2 positive tumor cells. These data indicate that the increase in NG2 positive cell number precedes oligodendroglioma formation. Furthermore, a NG2 positive cell fraction isolated from human grade II oligodendrogliomas can initiate oligodendroglioma formation in a mouse model, whereas NG2 negative cells are not capable of tumor formation. These data support that NG2 positive OPCs are the cell of origin for gliomas. However, the absence of multipotency and of the potential to form neurospheres indicates that these OPCs are not dedifferentiated into a more stem-like state39. In addition, in another study a model is used in which platelet-derived growth factor B (PDGF-B) drives the formation of oligodendrogliomas from OPCs. These oligodendrogliomas express OPC markers but lack the stem cell marker nestin. One third of the mice develop an oligodendroglioma, of which all 13 except one are low grade gliomas. These tumors have similar histological characteristics as human grade II oligodendrogliomas. These results point at restricted progenitors to be a possible origin of GSCs40. Experimental data also demonstrate that differentiated neurons and astrocytes are capable of glioma formation. Evidence comes for example from a mouse model in which nf1 and p53, two tumor suppressor genes which are often mutated in human glioblastoma, are silenced exclusively in neurons or astrocytes. This is achieved by injecting a lentiviral vector encoding short hairpin RNA (shRNA) for both nf1 and p53 in the brains of synapsin 1-cre transgenic or GFAP-cre transgenic mice to specifically target neurons or astrocytes respectively. Independent of whether the gene silencing occurs in either neurons or astrocytes, all mice develop glial tumors with histological characteristics resembling those of human glioblastomas. However, silencing of nf1 and p53 specifically in NSCs by using sox2-cre and nestin-cre transgenic mice also causes the formation of gliomas. When the tumors progress, the expression of stem cells and progenitor markers increases, while the expression of differentiation markers decreases. This most likely reflects the dedifferentiation of mature cells into stem or progenitor cells. The same results are obtained when cultured astrocytes from the mice in which nf1 and p53 are silenced are transplanted into NOD-SCID mice. Furthermore, when astrocytes or neurons in which nf1 and p53 are silenced are transferred from a culture with serum to a serumfree culture supplemented with FGF-2, the morphology of the cells alters and neurospheres are formed. Cells from these neurospheres express the stem cell markers sox2 and nestin. This study demonstrates that mature neurons and astrocytes can dedifferentiate into a cell with stem cell properties and that NSCs, mature neurons and mature astrocytes are capable of forming gliomas41. 3. EVIDENCE SUPPORTING THE HYPOTHESIS THAT GLIOMAS ARISE FROM GLIOMA STEM CELLS The identification of GSC in gliomas and the capacity of these cells to cause the formation and propagation of tumors in serial transplantation experiments in animal models supports the idea that the cancer stem cell hypothesis also applies to gliomas. However, the existence of GSCs and also the more general CSCs remains controversial and opinions about these stem cells range from questioning their existence to thinking about methods to target them in cancer therapy21. Thus, more evidence is required to make an evidence-based consideration about the role of GSCs in glioma pathogenesis. In this chapter, evidence for the existence of GSCs and their causal role in glioma formation are discussed. The niche in which stem cells reside is important for regulation of their self-renewal and differentiation29. Thus, studying GSCs in vivo in a developing tumor can be of great significance to elucidate the role of GSCs in the process of tumor formation and propagation. In a recent study, GSCs in developing high-grade gliomas are traced in living mice by multiphoton intravital microscopy. Surgically resected human high grade gliomas are divided into CD133 positive cell fractions (GSCs) and non-stem tumor cell fractions, which are transduced with lentiviruses to make the different fractions express different fluorescent proteins to allow tracing of these cells. The first and second week after transplantation of GSCs into the cortices of nude mice, the GSCs reside and grow in close proximity to blood vessels. In the third week a tumor appears and GSCs infiltrate the surrounding tissue (Fig. 5). 14 Moreover, when GSCs and non-stem tumor cells are transplanted into the cortices of nude mice in a ratio of 1:9, there is a rapid and strong increase in the volume occupied by GSCs, whereas the number of non-stem tumor cells slightly decreases. Thus, GSCs have a higher tumor forming potential than non-stem tumor cells. When the tumors are allowed to grow until the mice develop neurological signs, 94.5% of all tumor cells derives from the GSCs, whereas only 0.2% derives from non-stem tumor cells. This demonstrates that a large majority of the tumor cells are GSCs and GSCderived cells. Similarly as observed in human high-grade gliomas, GSCs and GSC-derived cells remain close to blood vessels. Moreover, 75% of the GSCs in culture prior to transplantation into the mouse brain, expresses the stem cell marker sox2, whereas only 25% of the GSCs expresses sox2 after transplantation. Thus, the cells that expressed sox2 in culture can generate other cell types in vivo. A decrease is also found in the cells expressing a marker for the M-phase of the cell cycle. These data suggest that only a subset of the GSCS is still capable of proliferating and that the in vivo environment regulates differentiation and thereby creates heterogeneity within the tumor. Together, these data demonstrate that GSCs are present in gliomas and are causal for tumor formation and propagation in vivo42. Fig. 5. Projection micrograph reveals green fluorescent protein (GFP) labeled GSCs (green) form a tumor close to dextran labeled blood vessels (red) at day 20 after transplantation in the cortex of nude mice. From: Lathia et al. 2011. Another experimental study supporting the hypothesis that gliomas arise from GSCs comes from a study in which the Sonic hedgehog (Ssh) pathway, which is a critical stem cell signaling pathway, is blocked by the compound cyclopamine. In glioma cell lines in which the Ssh pathway is activated, blockade causes decreased growth of the cells and when cells from dissociated neurospheres which received cyclopamine treatment are cultured in medium without the Ssh inhibitor, no neurosphere formation is detected. This demonstrates that inhibition of the Ssh pathway eliminates GSC from the tumor cells. Moreover, the number of GSCs increases following radiotherapy43, which is in line with the previous findings demonstrating an increase in CD133 positive cells after radiotherapy12. When human glioblastoma cells, which received cyclopamine treatment, are injected into the brains of athymic mice, no tumor is formed. Together, these data demonstrate that following Ssh blockade, which is a critical signaling pathway in stem cells, the GSCs are depleted43. Moreover, the cancer stem cell hypothesis implies that if GSC exist and if they are not removed, the tumor recurs. This is supported by the findings that following radiotherapy, the number of CD133 positive cells increases and that this subset of cells shows decreased apoptosis and increased activation of cell cycle checkpoint proteins to repair DNA damage12. Furthermore, when samples from primary and recurrent human glioblastomas are compared after receiving radio- and chemotherapy, the CD133 positive cell number is increased in recurrent tumors compared to primary tumors. In sections from primary glioblastomas, low proliferation levels are observed, whereas 15 higher proliferation is found in the recurrent samples. These data indicate that following therapy, CD133 positive cells survive and become highly proliferative and thereby the glioma regrows44. If GSCs are causal for the propagation of gliomas and an increase in stem cell properties means an increase in the stem cell state, it might be expected that expression of GSC markers correlates with disease prognosis. To assess this, markers for GSCs are required such as the transmembrane protein leucine-rich repeat containing G protein-coupled receptor 5 (LGR5), a recently identified marker of brain tumor stem cells including GSCs. LGR5 overexpression is detected in all glioma tissue samples and correlates to proliferation rates and the grade of the gliomas. Knockdown of LGR5 results in inhibition of the cell-cycle, subsequent inhibition of proliferation and decreased neurosphere formation in a glioma cell line. In vivo, cells in which LGR5 is inhibited show diminished tumor growth in a xenograft model. These results indicate that depletion of the GSC marker LGR5 causes a decrease in tumor forming potential, thus pointing at a possible role for GSCs in the formation of gliomas45. Evidence supporting the view that GSCs are crucial in glioma pathogenesis also comes from a study in which the role of zinc finger E-box binding homeobox 1 (ZEB1) in glioblastoma invasion and chemoresistance is examined. ZEB1 is mainly expressed by glioblastoma cells in the most infiltrative tumor area in xenograft mouse models. ZEB1 regulates MGMT on a transcriptional level by affecting microRNA-200c (miR-200c) and c-MYB, thereby causing infiltration of surrounding tissue and chemoresistance. The actions of ZEB1 lead to expression of the stem cell factors CD133, olig2 and sox2 and increased ZEB1 expression in a neurosphere assay causes an increase in sphere forming frequency. When ZEB1 is silenced with shRNA, tumor initiating capacity is diminished. Together, these data implicate that through activation the ZEB1 pathway, glioma cells have a higher capacity for tumor formation46. 4. RESEARCH TECHNIQUES TO INVESTIGATE GLIOMA STEM CELLS A GSC is defined by the ability to self-renew and produce a heterogeneous tumor mass. Identification of GSCs is based on the ability to form neurospheres, on the ability to differentiate into multiple cells types and on the ability to form a tumor in serial transplantation experiments resembling the original tumor phenotype. The latter characteristic distinguishes GSCs from normal NSCs19. Thus, cell culture and animal models are of great significance to assess these hallmarks of GSCs. This chapter will first highlight the most important in vitro techniques, followed by the most promising animal models. 4.1 IN VITRO MODELS FOR HUMAN GLIOMAS A very important tool in glioma research is culturing of glioma cells that are isolated from surgically removed human glioma tissue. The human tissue is dissociated and suspended and the tumor cells are cultured under serum-free conditions in the presence of FGF and EGF to promote GSC proliferation. GSCs can be distinguished from non-stem tumor cells based on their tendency to form neurospheres or by selecting for the stem cell marker CD133 with magnetic cell sorting18,27. GSC cultures can be maintained for about 20 passages without observing major changes in growth rates. However, new mutations are introduced especially at later passages, thus changing the genotype of the GSCs compared to the genotype of the tumor from which they are derived. The GSCs can differentiate when cultured under differentiation conditions47. The purified GSCs can be transplanted into immunocompromised mice to study the formation and propagation of the tumor. 16 Furthermore, several glioma cell lines which derive from human gliomas are available, such as U87 and U251. These cell lines are often used for transplantation into the brains of rodents. U251, which is one of the best studied glioma cell line, derives from a human glioblastoma48. When U251 cells are injected intracranially in nude mice, a glioma develops that displays necrosis, neovascularization, nuclear atypia and inflammation. However, the tumor displays no endothelial proliferation and does not always show signs of invasion of surrounding tissue49. The U87 cell line, which also derives from human glioblastoma, is mainly used to study neovascularization50. Tumors formed from U87 cells do not display necrosis, endothelial proliferation and do not always display invasion of surrounding tissue49. However, these cell lines are not suitable for studying GSCs, since they do not contain stem cells. Glioma stem cell lines include 9L, but this cell line shows less similarities with glioblastoma cells than the non-stem cell lines50. 4.2 IN VIVO MODELS FOR HUMAN GLIOMAS In vitro models remove the tumor cells from their niche and thus a critical component which provides the tumor with growth factors, oxygen and a matrix, is lacking29, whereas in vivo studies do include the interactions with the niche. Several vertebrate animal models for different types and grades of gliomas are available and many of these models involve mice. The two main types of mouse models are genetically engineered mouse models and xenograft mouse models. In genetically engineered mouse models, the mutations that are frequently found in human glioma tissue are induced in mice, thereby allowing the investigation of the causes and pathogenesis of gliomas in vivo48. Genetic mouse models have been developed for most genes known to be involved in human gliomas, for example mice which are heterozygous for tumor suppressor genes nf1, pten and p53. These mice develop high grade astrocytomas with 100% penetrance, show accelerated tumor formation and show decreased survival compared to mice heterozygous for only nf1 and p5351. Furthermore, genes can be controlled in a spatial manner with cre-mice, where for example the mutation is exclusively induced in GFAP-expressing cells48. In xenograft mouse models, glioma cells from human or murine glioma tissue or a glioma cell line are transplanted into the brains of mice. These mice are immunocompromised to avoid rejection of the xenograft. These models are predominantly used to study glioma pathogenesis and to test drugs 48. The NOD-SCID mouse model is frequently used, and injection of 100 CD133 positive cells is sufficient to induce glioma formation in this model18. Although some models are known in which the developing tumors show similar phenotypes as the human gliomas, not all the xenograft tumors are good representatives of the human tumors48. Recently, a new xenograft model for human gliomas was developed in pigs. Until now, the only large animal model for gliomas were dogs, but this model is difficult to use in experiments because the glioma develops spontaneously. This model is developed in pigs, since testing of continuous application of drugs over the blood-brain barrier by implanted devices is easier in large animals52 and because the anatomy of the brain is similar in pigs and humans53. In this pig xenograft model, cells of the human glioblastoma cell line U87 MG or the glioblastoma stem cell line G6, are implanted into the parietal lobe of the pigs, which are immunosuppressed by administration of ciclosporine. A glioma develops in about 95% of the animals which were transplantated with U87 MG cells, whereas only one out of 5 pigs transplanted with G6 cells develops a tumor. The tumor which is formed shows 17 angiogenesis, necrosis and infiltration of surrounding tissue and resembles the situation seen in human malignant gliomas. This can possibly be explained by the short follow-up period, because mice transplanted with G6 cells develop malignant gliomas slower than mice transplanted with U87 MG cells52. Recently an experimental setup to visualize GSCs in living mice by multiphoton intravital microscopy was developed. This technique allows tracing of individual cell types within a developing tumor42. In the future, this model could be expanded so that the volume occupied by GSCs before and after treatment can be compared. This model does not only have the potential to be an important model to study drug efficacy but also for providing the ultimate proof that GSCs are the cell of origin of gliomas, by observing that a therapy is effective in eliminating GSCs and improves the condition of the animals. Since animals are sacrificed after intravital microscopy, using different groups of animals from an identical strain might help to elucidate the role of GSCs in glioma pathogenesis. 5. REMAINING QUESTIONS AND CONCLUSION Although there an increasing number of studies showing the presence of GSCs in gliomas and confirming their causal role in glioma formation, there are still several remaining questions concerning the role of glioma stem cells in glioma formation. These questions are identified and discussed in this section. An important point of discussion is that the terms GSC and GIC are often confused and thereby complicates the debate. GICs are cells which undergo the initial cancerous transformation and are then able to initiate glioma formation. GSCs are the cells capable of self-renewal and maintaining a heterogeneous tumor. However, since GSCs can induce tumor formation in animal models, the terms are often confused. Thus, in the future it is important to gain more knowledge on both cell types to understand the remaining questions in the glioma stem cell field19. Another point of confusion are contrasting findings with the stem cell marker CD133. If CD133 expressing cells, which are considered to be stem cells, are causal for glioma propagation, it might be expected that the level of CD133 positive cells correlates with prognosis. This is investigated in several studies, although contradictory results are reported. For example, it is found that higher levels of CD133 are correlated with longer survival in glioblastoma patients after surgical resection and radiotherapy54. On the contrary, in several studies in which a combination of chemotherapy and radiotherapy are given, prognosis is worse in patients with high levels of CD13355. Related to this subject is that if gliomas arise from GSCs, it might be expected that high grade gliomas contain more GSCs than low grade gliomas. One study found that the number of CD133 expressing cells in a glioma is correlated to the WHO grade assigned to the glioma in patients with primary gliomas who did not receive radiotherapy or chemotherapy. No differences were found in the capacity for self-renewal or multipotency between the CD133 positive cell populations from gliomas of different grades in vitro. These data point at a role for CD133 expressing cells in glioma progression56. Moreover, it is also not clear if benign gliomas contain a stem cell population. Based on the glioma stem cell hypothesis, it might be assumed that benign gliomas lack GSCs because GSCs are causal for therapy resistance12 and cause the regrowth of gliomas44, which is not observed in low grade gliomas. One study failed to identify cells capable of neurosphere formation in grade I gliomas and grade II oligodendrogliomas after culturing these cells for 90 days in a serum-free culture system with EGF and FGF2, whereas 18 cells from high grade gliomas form neurospheres after 20 to 40 days in culture. These data indicate that low grade gliomas might not contain GSCs24. If the glioma hypothesis is true and GSC are crucial in glioma pathogenesis, GSC can arise from NSCs, more restricted PCs or mature astrocytes. This means that to provide evidence for the existence of GSCs and their role in glioma formation, is it crucial to have the appropriate markers to distinguish these cell types. At the moment, these markers are not yet available. CD133 is frequently used as GSC marker but the value is still controversial. One study reported that CD133 negative cells can also initiate tumor formation57, which is not in line with the findings from another study in which CD133 positive cells are shown to initiate tumor formation, whereas 500- to 1000-fold higher numbers of CD133 negative cells cannot18. Finding new markers for GSCs and other tumor cells and the possible cell types of origin of GSCs might help enormously in elucidating glioma pathogenesis. Also further investigation about the validity of current markers is needed. Gliomas can become resistant to radiotherapy12 and following surgical resection, gliomas often regrow28. Both approaches are focused at removing the majority of the cancer cells. According to the cancer stem cell hypothesis, only a small subset of the tumor cells, which are the GSCs, is capable of tumor formation and survival. This implicates that therapy which specifically targets the GSCs would be a more specific treatment for gliomas and might decrease recurrence and improve survival22. Thus, identification of the cell type responsible for glioma formation has major impact on therapy development and therefore research focusing on the glioma cell of origin is of huge importance14. To conclude, the experimental data discussed in this writing assignment provide a solid basis to support that the cancer stem cell hypothesis also applies to gliomas. The fact that both in vitro and in vivo studies confirm the causal role for GSCs in glioma formation strengthens the support for this hypothesis. The main problem now seems to be the lack of a valid GSC marker. When more selective markers are found to distinguish GSCs from NSCs and other cell types, this will help to answer the questions mentioned in this chapter. Thereby, it opens the way to show that future therapies, which selectively target GSCs, eliminate the tumor and improve outcome of glioma patients. This would be the ultimate proof for the causal role of GSCs in glioma formation21. Until then, the debate about the existence of GSCs and their role in glioma pathogenesis will be ongoing. 19 REFERENCES 1. Kumar, V., Abbas, A. K., Fausto, N. & Aster, J. Robbins & Cotran Pathologic Basis of Disease. (Elsevier, 2009). 2. Louis, D. N. et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 114, 97–109 (2007). 3. Houben, M. P. W. A. et al. Stable incidence of childhood and adult glioma in The Netherlands, 1989-2003. Acta Oncol. 45, 272–9 (2006). 4. Crocetti, E. et al. Epidemiology of glial and non-glial brain tumours in Europe. Eur. J. Cancer 48, 1532–42 (2012). 5. Sant, M. et al. Survival of European patients with central nervous system tumors. Int. J. cancer 131, 173–85 (2012). 6. Jackson, R. J. et al. Limitations of stereotactic biopsy in the initial management of gliomas. Neuro. Oncol. 3, 193–200 (2001). 7. Weller, M. et al. Personalized care in neuro-oncology coming of age: why we need MGMT and 1p/19q testing for malignant glioma patients in clinical practice. Neuro. Oncol. 14 (Suppl, iv100–iv108 (2012). 8. Paz, M. F. et al. CpG Island Hypermethylation of the DNA Repair Enzyme Methyltransferase Predicts Response to Temozolomide in Primary Gliomas. Clin. cancer Res. 10, 4933–4938 (2004). 9. Grasbon-Frodl, E. M. et al. Intratumoral homogeneity of MGMT promoter hypermethylation as demonstrated in serial stereotactic specimens from anaplastic astrocytomas and glioblastomas. Int. J. cancer 121, 2458–64 (2007). 10. Yabroff, K. R., Harlan, L., Zeruto, C., Abrams, J. & Mann, B. Patterns of care and survival for patients with glioblastoma multiforme diagnosed during 2006. Neuro. Oncol. 14, 351–359 (2012). 11. Juratli, T. a, Schackert, G. & Krex, D. Current status of local therapy in malignant gliomas - a clinical review of three selected approaches. Pharmacol. Ther. 139, 341–58 (2013). 12. Bao, S. et al. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature 444, 756–60 (2006). 13. Kaufmann, J. K. & Chiocca, E. A. Glioma virus therapies between bench and bedside. Neuro. Oncol. 16, 334–351 (2014). 14. Florio, T. & Barbieri, F. The status of the art of human malignant glioma management: the promising role of targeting tumor-initiating cells. Drug Discov. Today 17, 1103–10 (2012). 15. Reya, T., Morrison, S. J., Clarke, M. F. & Weissman, I. L. Stem cells, cancer, and cancer stem cells. Nature 414, 105–11 (2001). 20 16. Clarke, M. F. et al. Cancer stem cells--perspectives on current status and future directions: AACR Workshop on cancer stem cells. Cancer Res. 66, 9339–44 (2006). 17. Chen, J., McKay, R. M. & Parada, L. F. Malignant glioma: lessons from genomics, mouse models, and stem cells. Cell 149, 36–47 (2012). 18. Singh, S. K. et al. Identification of human brain tumour initiating cells. Nature 432, 396–401 (2004). 19. Sampetrean, O. & Saya, H. Characteristics of glioma stem cells. Brain Tumor Pathol. 30, 209– 14 (2013). 20. Shackleton, M., Quintana, E., Fearon, E. R. & Morrison, S. J. Heterogeneity in cancer: cancer stem cells versus clonal evolution. Cell 138, 822–9 (2009). 21. Jordan, C. T. Cancer stem cells: controversial or just misunderstood? Cell Stem Cell 4, 203–5 (2009). 22. Stiles, C. D. & Rowitch, D. H. Glioma stem cells: a midterm exam. Neuron 58, 832–46 (2008). 23. Siebzehnrubl, F. A., Reynolds, B. a, Vescovi, A., Steindler, D. a & Deleyrolle, L. P. The origins of glioma: E Pluribus Unum? Glia 59, 1135–47 (2011). 24. Galli, R. et al. Isolation and Characterization of Tumorigenic, Stem-like Neural Precursors from Human Glioblastoma. Cancer Res. 64, 7011–7021 (2004). 25. Ignatova, T. N. et al. Human cortical glial tumors contain neural stem-like cells expressing astroglial and neuronal markers in vitro. Glia 39, 193–206 (2002). 26. Uchida, N. et al. Direct isolation of human central nervous system stem cells. Proc. Natl. Acad. Sci. U. S. A. 97, 14720–14725 (2000). 27. Singh, S. K. et al. Identification of a Cancer Stem Cell in Human Brain Tumors. Cancer Res. 63, 5821–5828 (2003). 28. Oppitz, U., Maessen, D., Zunterer, H., Richter, S. & Flentje, M. 3D-recurrence-patterns of glioblastomas after CT-planned postoperative irradiation. Radiother. Oncol. 53, 53–7 (1999). 29. Tavazoie, M. et al. A specialized vascular niche for adult neural stem cells. Cell Stem Cell 3, 279–88 (2008). 30. Dirks, P. B. Brain tumor stem cells: the cancer stem cell hypothesis writ large. Mol. Oncol. 4, 420–30 (2010). 31. Eriksson, P. S. et al. Neurogenesis in the adult human hippocampus. Nat. Med. 4, 1313–7 (1998). 32. Doetsch, F., Caillé, I., Lim, D. a, García-Verdugo, J. M. & Alvarez-Buylla, a. Subventricular zone astrocytes are neural stem cells in the adult mammalian brain. Cell 97, 703–16 (1999). 21 33. Kukekov, V. G. et al. Multipotent stem/progenitor cells with similar properties arise from two neurogenic regions of adult human brain. Exp. Neurol. 156, 333–44 (1999). 34. Seri, B., García-Verdugo, J. M., McEwen, B. S. & Alvarez-Buylla, A. Astrocytes give rise to new neurons in the adult mammalian hippocampus. J. Neurosci. 21, 7153–60 (2001). 35. Menn, B. et al. Origin of oligodendrocytes in the subventricular zone of the adult brain. J. Neurosci. 26, 7907–18 (2006). 36. Quiñones-Hinojosa, A. et al. Cellular composition and cytoarchitecture of the adult human subventricular zone: a niche of neural stem cells. J. Comp. Neurol. 494, 415–34 (2006). 37. Leonard, B. W. et al. Subventricular Zone Neural Progenitors from Rapid Brain Autopsies of Elderly Subjects with and without Neurodegenerative Disease. J. Comp. Neurol. 515, 269–294 (2009). 38. Alcantara Llaguno, S. et al. Malignant astrocytomas originate from neural stem/progenitor cells in a somatic tumor suppressor mouse model. Cancer Cell 15, 45–56 (2009). 39. Persson, A. I. et al. Non-stem cell origin for oligodendroglioma. Cancer Cell 18, 669–82 (2010). 40. Lindberg, N., Kastemar, M., Olofsson, T., Smits, a & Uhrbom, L. Oligodendrocyte progenitor cells can act as cell of origin for experimental glioma. Oncogene 28, 2266–75 (2009). 41. Friedmann-Morvinski, D. et al. Dedifferentiation of neurons and astrocytes by oncogenes can induce gliomas in mice. Science 338, 1080–4 (2012). 42. Lathia, J. D. et al. Direct in vivo evidence for tumor propagation by glioblastoma cancer stem cells. PLoS One 6, e24807 (2011). 43. Bar, E. E. et al. Cyclopamine-mediated hedgehog pathway inhibition depletes stem-like cancer cells in glioblastoma. Stem Cells 25, 2524–2533 (2007). 44. Tamura, K. et al. Expansion of CD133-positive glioma cells in recurrent de novo glioblastomas after radiotherapy and chemotherapy. J. Neurosurg. 119, 1145–55 (2013). 45. Wang, D. et al. Knockdown of LGR5 suppresses the proliferation of glioma cells in vitro and in vivo. Oncol. Rep. 31, 41–9 (2014). 46. Siebzehnrubl, F. a et al. The ZEB1 pathway links glioblastoma initiation, invasion and chemoresistance. EMBO Mol. Med. 5, 1196–1212 (2013). 47. Pollard, S. M. et al. Glioma stem cell lines expanded in adherent culture have tumor-specific phenotypes and are suitable for chemical and genetic screens. Cell Stem Cell 4, 568–80 (2009). 48. Chen, L., Zhang, Y., Yang, J., Hagan, J. P. & Li, M. Vertebrate animal models of glioma: understanding the mechanisms and developing new therapies. Biochim. Biophys. Acta 1836, 158–65 (2013). 22 49. Candolfi, M. et al. Intracranial glioblastoma models in preclinical neuro-oncology: neuropathological characterization and tumor progression. J. Neurooncol. 85, 133–48 (2007). 50. Jacobs, V. L., Valdes, P. a, Hickey, W. F. & De Leo, J. a. Current review of in vivo GBM rodent models: emphasis on the CNS-1 tumour model. ASN Neuro 3, e00063 (2011). 51. Kwon, C.-H. et al. Pten haploinsufficiency accelerates formation of high-grade astrocytomas. Cancer Res. 68, 3286–94 (2008). 52. Selek, L. et al. Imaging and histological characterization of a human brain xenograft in pig: the first induced glioma model in a large animal. J. Neurosci. Methods 221, 159–65 (2014). 53. Lind, N. M. et al. The use of pigs in neuroscience: modeling brain disorders. Neurosci. Biobehav. Rev. 31, 728–51 (2007). 54. Kase, M. et al. Impact of CD133 positive stem cell proportion on survival in patients with glioblastoma multiforme. Radiol. Oncol. 47, 405–10 (2013). 55. Dahlrot, R. H., Hermansen, S. K., Hansen, S. & Kristensen, B. W. What is the clinical value of cancer stem cell markers in gliomas? Int. J. Clin. Exp. Pathol. 6, 334–48 (2013). 56. Thon, N. et al. Presence of pluripotent CD133+ cells correlates with malignancy of gliomas. Mol. Cell. Neurosci. 43, 51–59 (2010). 57. Nishide, K., Nakatani, Y., Kiyonari, H. & Kondo, T. Glioblastoma formation from cell population depleted of Prominin1-expressing cells. PLoS One 4, e6869 (2009). 23