LOs week 3 - Embryology (Sylvie) - PBL-J-2015
advertisement
 - PBL-J-2015")
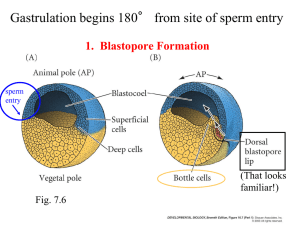
Anatomy: Human development- embryology NB: Really good website for all this stuff is: http://www.embryology.ch/genericpages/moduleembryoen.html - I would just look at this to be honest! Understand the anatomical features of o the male and female gametes and o The male and female reproductive tracts enzymes Motile, uses lots of ATP. Tail provides propulsion Stationary Lots of nutrients, large cytoplasm ATP from mitochon dria HAPLOID Genetic material, including either X or Y sex chromosome HAPLOID Genetic material, with only X sex chromosome Secretions Semen = sperm + secretions Activates sperm Sperm produced here Stores sperm – 13 m long Fertilisation most often occurs in the fallopian tube. Then the fertilized egg travels down and embeds in the uterine wall. If it doesn’t migrate it’s called an ectopic pregnancy and must be aborted to avoid permananent damage or death of the mother Endometrial epithelium = single layered prismatic epithelium of uterus Endometrium = inner lining of uterus, where zygote embeds Myometrium = muscular layer of uterus Overview of fertilization http://www.embryology.ch/anglais/bvueEmbr/evorimplantation/03.html Time after fert. 24 hours Day 4 Developmental stage Characteristics Location Zygote After fertilization and before cleavage Morula After cleavage. ‘Ball’ of blastomeres Day 6 Blastocyst Day 8 Day12 Complete implantation Embryonic disc undergoes gastrulation Day 21 Axial canal formed Day 23 Notochord separates Cells differentiate into embryoblast and trophoblast Cytotrophoblast, syncytiotrohphoblast, epiblast and hypoblast Bilaminar embryonic disc. The epiblast (upper layer) → 3 layers endoderm, ectoderm and mesoderm. GASTRULATION Invagination of epiblast cells migrate from primitive node Notochord is separated now Fallopian tube at ampulla Travelling down fallopian tube Uterine wall Endometrium Attached to endometrium by a connecting stalk “” “” NB: The embryonic period comprises the first 8 weeks of pregnancy. It is divided into a preembryonic phase (from the 1rst to the 3rd week), in which the three germinal layers arise, and into the embryonic phase proper (from the 4th to 8th week), in which the embryonic organ anlagen arise. Understand the process of fertilization 1 2 3 4 5 6 Stage of fertilization Sperm goes through corona radiata Penetration of zona pellucida Fusion of plasma membranes of oocyte and sperm Oocyte undergoes 2nd meiotic division. AND formation of female pronucleus Formation of male pronucleus Zygote is formed! Description Acrosome releases enzymes, which digest the corona radiata until the sperm reaches the zona pellucida Acrosomal enzymes again digest – this time the enzyme is acrosin. A reaction occurs that prevents any other sperm entering the egg (oocyte) – the zona pellucida is made impermeable Plasma membranes fuse, but nuclear (genetic) fusion hasn’t yet occurred. Ova are suspended after Meiosis 1, and so when the oocyte is fertilized by the sperm it undergoes Meiosis 2 - Just a thing you need to remember. The sperm has already completed Meiosis 2. Haploid nucleus of sperm contains either X or Y sex chromosome, therefore father determines sex of offspring (oocyte always contains X). Fusion of the pronuclei creates a new DIPLOID zygote, with 46 chromosomes, half contributed from the oocyte (mother) and half contributed from the sperm (father) Know the terms: 1. Zygote noun: A diploid (2n i.e. 46 chromosomes) cell formed from the fusion of two haploid (n i.e. 23 chromosomes) gametes: the sperm fertilising the egg. This very early stage lasts until the first cleavage. NB: Cleavage is repeated mitotic cell divisions. The dividing cells are called blastomeres. 2. Morula noun from the Latin for ‘mulberry’: After the first cleavage, it’s called a morula. It’s a ball of 16-32 blastomeres which are also considered stem cells, as they are undifferentiated cells and could potentially become any cell in the body. This stage lasts until blastocyst formation. 3. Blastocyst noun: A hollow, thin-walled structure containing a cluster of cells called the embryoblast (or inner cell mass) which will become the embryo. The outer layer (trophoblast) of the blastocyst will become the placenta and other supporting tissues. A blastocyst contains some cells that have differentiated (changed). Explain the process of implantation of the blastocyst . The blastocyst attaches itself to the uterine wall, on the endometrial epithelium. Below the endometrial epithelium in the endometrium itself are capillaries and endometrial glands. These two structures supply blood (O2) and secrete required nutrients respectively. The trophoblast (‘troph’ means relating to nutrition and feeding) digests the uterine wall, and transports the nutrients it obtains back into the blastocyst. The trophoblast is now composed of two layers: The syncytiotroblast – invades the endometrial connective tissue and interrupts the menstrual cycle by releasing beta hCG. This is picked up by early pregnancy tests and indicates the embryo has implanted. The cytotrophoblast – covers the embryo The embryo uses these two structures to completely embed itself in the uterine wall. The embryoblast differentiates into a two-layered embryonic disc Hypoblast – support structure Epiblast – actually becomes the baby Understand the development of the ectoderm, endoderm + mesoderm. Gastrulation (“formation of the gut”) 1. Blastula → 2. Gastrula with different germ layers Blastocyst becomes a gastrula. A gastrula is a trilaminar (three-layered) stage of embryo development, where the three germ layers are endoderm, ectoderm and mesoderm. The embryonic disc (remember it’s bilaminar i.e. epiblast and hypoblast) undergoes these changes: 1. Loss of symmetry 2 Formation of primitive streak 3 Epithelial cells become endoderm, ectoderm and mesoderm Formation of proximal-distal (caudal-cranial) and anterior-posterior axes. Direction signaled by nodal signalling Forms from ‘caudal’ or proximal end and grows towards ‘cranial’ or distal end. This establishes the bilateral symmetry of the embryo. The caudal or proximal end will be the ‘tail’ end of the embryo (caudal – tail-like) Along the primitive streak epithelial cells migrate down inside the embryo to become a new layer, called the endoderm, pushing the hypoblast out of the way (this goes on to form the amnion.) The epiblast keeps moving and forms a second layer, the mesoderm. The top layer is now called the ectoderm. Summary of what’s just happened to the embryonic disc: Embryonic disc is bilaminar, it has two layers: Epiblast → primitive streak and ectoderm → endoderm → mesoderm Hypoblast → endoderm of umbilical vesicle → extraembryonic mesoderm (i.e. support structures) What do these three newly formed layers of the embryo become? Ectoderm Epidermis Central and peripheral nervous systems Eye Inner ear Mesoderm Skeletal muscles Blood cells and lining of blood vessels Smooth muscle Cardiovascular system Bones, tendons and ligaments Dermis Endoderm epithelial lining of gastrointestinal tract Epithelial lining of respiratory tract Some glandular cells This is what the whole structure looks like at this point: Formed from epiblast Formed from hypoblast Understand the development of the notochord and explain its significance Overview: http://embryology.med.unsw.edu.au/Medicine/BGDlabfertilization10.htm The notochordal process begins as a fold of ectoderm extending cranially. The sequence of differentiation: Notochordal process → notochordal plate → notochord. It occurs during GASTRULATION: “Migrating cells produce a thick knob at one end of the primitive streak. Their continued forward movement from this so-called primitive knot [node] produces a dense band that becomes the rodlike notochord” – encyclopedia Brittanica http://www.britannica.com/EBchecked/topic/474953/prenatal-development/63787/Formation-of-the-three-primary-germlayers?anchor=ref526542 In detail: The notochordal process elongates by invagination from the primitive pit. It’s a hollow tube called the notochordal canal ventral to (under) the ectoderm. It then forms a notochordal plate which is continuous with the endoderm. Finally the notochordal plate in-folds and forms the notochord. The notochord regulates cellular differentiation. It plays an organisational role in central nervous system development. It will later become part of the vertebral column. This is different to the process that creates the neural tube. The notochord induces the differentiation of the neuroblast. This process is called neurulation. The median part of the epiblast thickens and forms a groove and afterwards a tube (neural tube), out of which the central nervous system will arise. From http://www.embryology.ch/anglais/bvueEmbr/vueembryo.html Understand the relationship of fertility to the patency of the fallopian tube Patent fallopian tubes = unblocked or open The fallopian tube is much more complex than a simple pipe, and the lining of the tube is folded and lined with microscopic hair like projections called cilia which push the egg and embryo along the tube. Any factor that affects the motility or patency of the fallopian tube can cause infertility. Tubal disease has been implicated in 15-20% of couples presenting with infertility. Tubal damage usually occurs through pelvic infection, and this is called pelvic inflammatory disease (PID). This causes the fallopian tubes to lose patency. Some of the causes of pelvic infection that can be pinpointed are: Sexually transmitted diseases (e.g. Gonorrhea, Chlamydia) Infection after childbirth, miscarriage, termination of pregnancy ( MTP) or IUD (intrauterine device) insertion Post-operative pelvic infection (e.g. perforated appendix, ovarian cysts) Severe endometriosis Tuberculosis Besides causing blocked tubes, any pelvic inflammatory disease can also produce bands of scar tissue called adhesions, which can alter the functioning of the fallopian tubes. From http://www.drmalpani.com/book/chapter12a.html And http://www.trichurheart.com/images/Infertility.pdf