CaseStudyReport
advertisement

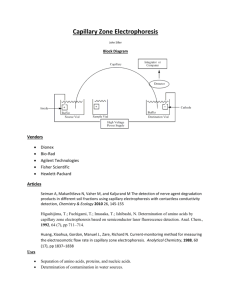
California State Polytechnic University, Pomona Chemical & Materials Engineering Department CHE 313: Transport Modeling CASE STUDY Oxygen Transport from a Perfluorocarbon Blood Substitute May 25, 2012 by Souza, Betty E. This case study is given under the Honor System and by signing here I have agreed that the work submitted is my work alone and that I neither sought nor received help from others. Presentation 20% Model Development 25% Solution 25% Discussion 20% Completeness and Neatness 10% February 6, 2016 Dr. T.K. Nguyen Chemical engineering Department California State Polytechnic University, Pomona 3801 West Temple Avenue Pomona, CA 91768 Dr. Nguyen: I have researched the development and use of artificial blood products for the ChE 313 case study. I have developed and solved a model for oxygen transport in the capillaries and tissues for a perfluorocarbon emulsion used as a blood substitute. As the shortage of blood is a pressing concern in this country and world wide, this seems to be an important area of study. The development of a substitute for blood is difficult because of the human body’s tendency to reject or destroy any foreign materials. This has been a problem in developing a hemoglobin based blood substitute. Perfluorocarbons (PFCs) are organic compounds similar to Teflon. They are inert and therefore not rejected or attacked by the body’s immune system. PFCs are good oxygen carriers and several PFC blood substitutes are being developed and tested. Following the oxygen transport model developed for natural blood in the Fournier text, I have developed and solved a model for the transport of oxygen in the capillaries and tissue for the case when PFC is used as a blood substitute. Figure 1 illustrates the capillary and tissue system of interest. The model for PFC is much the same as that for natural blood with the exception of the parameter m. This difference is outlined in the model development. Figure 2 shows a comparison of the oxygen profile for natural blood and PFC with identical inlet oxygen concentrations. The profiles are very similar. As expected, the profile for PFC is steeper than that for natural blood. This is reasonable because PFC will release its oxygen more readily into the plasma than will hemoglobin, making more oxygen available for transport to the tissues, and depleting the oxygen more quickly. The amount of oxygen absorbed by PFCs is directly proportional to the oxygen available for transfer in the lungs. To illustrate the effects of this phenomenon, I have graphed (figure 3) the resulting oxygen profiles for the case when the entering PFC PO2 is about half and one and a half times the nominal value assumed for arterial blood PO2. This graph shows that anoxia is an issue at inlet concentrations less than the nominal value. Given that blood transfusions do not replace all of a patients blood, I have also calculated the oxygen profiles for a 1:1 mixture of natural blood and PFC at various inlet oxygen concentrations. The results of this analysis can be found in figures 4, 5, and 6. Analysis of the results of this model for oxygen transport from PFC shows that if initial oxygen concentration of the blood stream can be kept slightly above that for natural blood, PFC will be an effective in carrying oxygen to the various tissues in the body. Sincerely, Betty Souza Background Each year, in the United States alone, about 12 million units (6 million liters) of blood is transfused, and worldwide demand is estimated to increase by 7.5 million liters per year. It is predicted that by the year 2030 the United States will be experiencing a shortage of 2 million liters per year. This shortage is due to low overall donation rates – only about 5% of Americans donate blood --, a short shelf life for donated blood, and difficulty finding perfectly matched blood (Nucci). The search is on for an artificial blood product that can make up this shortfall as well as solve some other problems encountered when transfusing blood. Ideally a blood substitute would be acceptable to patients of all blood types, nontoxic, have a long shelf life with minimal storage restrictions, stay in the blood stream long enough for the patient to rebuild their own blood, and be a good oxygen carrier (Nucci). Natural blood transports oxygen by way of hemoglobin molecules within the red blood cells (RBC). Each milliliter of human blood contains about 5 million red blood cells, each of which contain about 250 million molecules of hemoglobin. Each molecule of hemoglobin can transport a maximum of 4 molecules of oxygen from the lungs to various parts of the body. Each RBC also contains 2,3diphosphoglycerate (2,3-DPG). 2,3-DPG is a compound that makes it possible for hemoglobin to release its oxygen throughout the body and it also prevents auto-oxidation and the breakdown of the hemoglobin. In addition to transporting oxygen from the lungs, hemoglobin can bind with carbon dioxide and transport it back to the lungs to be exhaled (Nucci). More than half a dozen biotechnology companies have developed products designed to replicate the role of hemoglobin in the blood. These products generally fall into two classes; synthetic oxygen carriers and hemoglobin based blood substitutes. Hemoglobin based substitutes utilize human hemoglobin from outdated donated blood or hemoglobin from animals. Hemoglobin cannot be transfused without the protection of the RBC, because naked hemoglobin breaks down rapidly and is toxic to the kidneys. Proposed solutions include the encapsulation of hemoglobin in liposomes, attaching polyethylene glycol to the molecule to protect it in a shell of water, and polymerizing the molecule to strengthen its bonds (Lawton). So far, none of the hemoglobin-based products is commercially available. Clinical trials of Baxter Healthcare’s HemAssist blood substitute were halted in April 1998 when death rates due to an increase in blood pressure exceeded projections (AP). Perfluorocarbons (PFCs), synthetic organic compounds similar in composition to Teflon, are the most effective class of synthetic oxygen carriers (Lawton). PFCs will not dissolve in plasma but can be emulsified with various agents that allow them to be dispersed as tiny particles in the blood. They deliver gas passively and absorb oxygen preferentially over RBCs. They also release oxygen more quickly into the blood plasma since they are not housed inside a cell membrane (Nucci). Unlike hemoglobin, the amount of oxygen PFCs can carry is directly proportional to the oxygen available to them in the lungs. The drawback to PFCs, as stated by Dr. Winslow of UC San Diego, is that their “oxygen carrying capacity is so low that patients have to breathe pure oxygen” to make them effective (Lawton). While several PFC based products have made it to clinical trials, storage and effectiveness issues have kept them from experiencing much success. The following model will attempt to predict the average oxygen profile in the capillary and at the tissue cylinder radius when a PFC based blood substitute is used as compared to natural blood. I will follow the model development for oxygen transport from natural blood in the Krogh tissue cylinder model presented in the Fournier reference. In this model, oxygen is released from the hemoglobin into the plasma, and only the oxygen in the plasma can diffuse into the surrounding tissue. Only minor modifications to this model will need to be made to simulate the oxygen transport by PFCs. It has been noted that blood transfusions are required when more than 40% of the total volume is lost (Nucci). I will therefore model the oxygen profile for the cases of 100% natural blood, 100% PFC, and a 1:1 ratio of natural blood to PFC. Oxygen Transport Model Development To develop the model for oxygen transport from the capillary to the tissues, we will use a shell balance and the Krogh tissue cylinder model. The Krogh tissue cylinder model is a simplified model of the tissue surrounding the capillary. It assumes a cylindrical layer of tissue surrounding each capillary, that is fed from only that capillary (Fournier, 44). The capillary is assumed to be cylindrical and of constant radius. Three shell balances will be completed to describe the transport of oxygen bound to hemoglobin, oxygen dissolved in the plasma, and oxygen in the tissue. These balances will then be combined and simplified to complete the model for oxygen transport. Shell balance on hemoglobin bound oxygen in the capillary: Variables: C’ = concentration of oxygen in capillary that is bound to hemoglobin. V = Average velocity of blood in the capillary RHb0 = Production rate of oxygenated hemoglobin r = distance in radial direction z = distance in direction of flow 2rrzC ' 2rrVC ' z 2rrVC ' t z z RHbO 2rrz The first two terms on the right side of this equation represent the convective transport of oxygen. No diffusive transport terms are include in this balance since the oxygen is bound to hemoglobin (which is enclosed in the red blood cells and travels with the flow of blood) and is not free to diffuse. Dividing by 2rrz and taking the limit as z 0 gives: C ' C ' V R HbO t z Shell balance on dissolved oxygen in the capillary: Variables: C = concentration of oxygen in dissolved in capillary V = Average velocity of blood in the capillary D = diffusivity of oxygen in bloodstream rc = radius of capillary Roxygen = Production rate of oxygen in the bloodstream r = distance in radial direction z = distance in direction of flow 2rrzC 2rrVC z 2rrVC t C 2rr D z z z z 2rz D C r 2rr D C z z z r C 2rz r r r Roxygen 2rrz The first bracketed term is the convective mass transport of the dissolved oxygen. The second bracketed term is the diffusive mass transport in the radial direction, and the third bracketed term is the diffusive mass transport in the axial direction. Dividing by 2rrz and taking the limit as z 0 and r 0 gives: 1 C 2 C C C V D r 2 Roxygen t r r r r z We can now simplify and combine these two balances by noting the following: C ' C ' C C m t C t t C ' C ' C C m z C z z where m = dC’/dC RHbO = - Roxygen by Henry’s law, PO2=HC where PO2 =partial pressure of O2 and H=Henry’s constant This gives us a combined balance on oxygen dissolved in the plasma and bound to hemoglobin as follows: 1 m 1 PO 2 2 PO 2 PO 2 P V 1 m O 2 D r 2 t z r r r z (Equation A) Shell balance on dissolved oxygen in the tissue: Variables: CT = concentration of dissolved oxygen in tissue DT = diffusivity of oxygen in tissue rT = radius of tissue cylinder metabolic = Volumetric oxygen consumption rate in tissue r = distance in radial direction z = distance in direction of flow T C T T C 2rrzC T 2rz D T 2 r z D r r r t r r T C T T C 2rr D T 2 r r D z z z z z metabolic 2rrz The first bracketed term is the diffusive mass transport in the radial direction, and the second bracketed term is the diffusive mass transport in the axial direction. Dividing by 2rrz and taking the limit as z 0 and r 0 , and again noting that PTO2=HCT where PTO2 is the partial pressure of oxygen in the tissue: POT2 POT2 T 1 r D t r r r 2 POT2 T z 2 metabolicH (Equation B) Equations A & B can be further simplified with the following Additional Assumptions: 1) steady state conditions – neglect all time derivatives 2) axial diffusion of O2 in bloodstream negligible compared to convective transfer 3) since radial dimensions of tissue region much less than axial dimensions, axial diffusion in the tissue can be ignored 4) negligible concentration gradients in the radial direction within the capillary, and radially average the capillary oxygen levels – this is illustrated below resulting equations: POT2 rmetabolicH T / D T r r r 1 PO 2 P V 1 m O 2 D r z r r r (Equation B2) (Equation A2) To find the average radial PO2, we integrate equation A2 over the r direction rc 2 1 mV 0 2 1 mV rc PO 2 1 P rdr 2D r O 2 z r r r 0 rc PO 2 d P r dr 2 Dr O 2 c dz 0 r rdr rc rc Recognizing that the average PO2 can be defined as PO 2 rc2 2 PO 2 rdr , the 0 above equation becomes 1 m d PO 2 dz 2 D dPO 2 rcV dr rc Further assuming that the capillary wall provides negligible resistance to mass transfer, so that the oxygen flux at rc is continuous, 1 m d PO 2 dz 2 D T dPO 2 rcV dr rc (Equation A3) Analytical solutions for oxygen profiles in capillary and tissue regions: Tissue: POT2 r r r rmetabolicH T / D T Boundary conditions: (Equation B2) @ r = rc POT2 PO 2 @r = rT dPOT2 0 dr Integrating twice gives: r 2 HT r 1 P r , z PO 2 z c metabolic 4D T rc T O2 2 r 2 HT r T metabolic ln 2D T rc (Equation B3) Capillary: 1 m d PO 2 dz T 2 D T dPO 2 rcV dr rc (Equation A3) To solve for this equation for the oxygen profile in the capillary PO2 z , we need dPOT2 rc . We can differentiate equation B3 with respect to r to dr T metabolicH T rc rT2 T dPO 2 2 1 . obtain: D rc r dr 2 c Substituting this back into equation A3 and integrating gives: to evaluate D T PO 2 z PO 2 metabolicH T in 1 mV r T rc 2 1 z (Equation A4) Equations A4 and B3 can be used to determine the oxygen profile in the capillary or in the tissue region. These equations can be applied to natural blood or an artificial oxygen carrier by correctly evaluating the parameter m. POn2 C' For blood, recognizing that Y , C ' sat P50n POn2 n 1 m PO 2 dC ' dY dY C ' sat HC ' sat nP50n HC ' sat dC dC dPO 2 P50n POn2 For the artificial oxygen carrier PFC, m dC ' dC d 2 PO 2 T H PFC H P H PFC d OT2 H Tissue Membrane O2 O2 O2 O2 O2 O2 O2 O2 O2 O2 O2 O2 Capillary O2 O2 O2 O2 O2 O2 O2 O2 O2 O2 Flow O2 O2 Tissue Hemoglobin or artificial oxygen carrier Plasma This figure illustrates hemoglobin or an artificial oxygen carrier flowing in the plasma. Oxygen is released from the oxygen carrier to the plasma. Oxygen dissolved in the plasma is then transported across the capillary wall to the tissues. Figure 1 Results and Discussion Several assumptions were made in the development of the oxygen transport equations that will cause the values in figures 2 through 4 to be overstated. Radial diffusion in the capillary has been partially neglected by averaging the radial concentration. Resistance to diffusion through the capillary wall has been neglected. Since oxygen is such a small molecule, neglecting this resistance should not cause a significant error. The values for the physical properties used to obtain solutions for this model were values given for the similar model in the Fournier reference. The tissue perfusion rate of 0.7 ml/cm3*min is the given value for the blood perfusion rate to the heart. The assumed exit PO2 level of 31mmHg has been verified by the calculations for PO2(z) at the capillary exit (30.9mmHg). All oxygen values given for the tissue region are at the outside radius of the tissue cylinder. For the given physical values, Figure 2 shows that for natural blood, no anoxic regions exist in the capillary or tissue. For PFC at PO2in = 95mmHg, the tissue becomes anoxic at about z=. 088cm. The partial pressure of oxygen at the entrance to the capillary was also evaluated at 45mmHg and 145mmHg to simulate the possibility of the patient receiving less than or more than the ideal amount of oxygen during transfusion. Figure 3 illustrates that at 45mmHg, The tissue becomes anoxic after the PFC has traveled only about 30% of the way down the capillary. The fluid in the capillary will become anoxic at about 0.055cm. This illustrates the need to keep the patient well oxygenated while using this product. The oxygen profiles were also evaluated for the case of a 1:1 mixture of PFCs and natural blood. I evaluated these mixtures with PO2in for blood constant at 95mmHg, and allowed the PO2in for PFC to vary from 45mmHg to 145mmHg. I have insufficient data to determine the relationship between blood and PFC P O2 levels. For the case of PO2in=45mmHg, it does seem reasonable that since PFC can give up its oxygen so easily, there would be a lower concentration in the blood due to the PFC as compared to natural blood. The fact that PFC absorbs oxygen in the lungs in preference to the red blood cells gives credence to the possibility that the concentration of O2 in the blood due to PFC could exceed that due to natural blood. Either case would be contingent on the concentration of O 2 available in the lungs. Figures 4,5, and 6 compare the oxygen profiles for the combination of blood and PFC to natural blood at PO2in=95mmHg. Figure 4 shows that for both components having a PO2in=95mmHg the tissue just becomes anoxic at the corner of the cylinder where z=L. Figure 5 shows no anoxic region, but there is the possibility of tissue damage from over oxygenation. Figure 6 shows significant anoxic regions in the tissue at PFC PO2in=45mmHg. 120.0 Partial Pressure Oxygen (mmHg) 100.0 Bloodcapillary blood-tissue 80.0 60.0 40.0 20.0 0.0 0.000 0.020 0.040 0.060 0.080 0.100 0.120 -20.0 Distance (cm) Figure 2. Partial Pressure of Oxygen vs. distance along capillary (PO2in = 95 mmHg) Partial Pressure of Oxygen (mmHg) 200.0 95mmHg-capillary 95mmHg-Tissue 145mmHg-capillary 145mmHg-tissue 45mmHg-capillary 45mmHg-Tissue 150.0 100.0 50.0 0.0 0.000 0.020 0.040 0.060 0.080 -50.0 -100.0 Distance (cm) Figure 3. Oxygen Profile for PFC 0.100 0.120 Partial Pressure O2 (mmHg) 100.0 blood- capillary 80.0 blood - tissue 60.0 40.0 20.0 0.0 0.000 0.020 0.040 0.060 0.080 0.100 0.120 -20.0 Distance (cm) Figure 4. Partial Pressure of Oxygen vs. distance along capillary (Blood and PFC 1:1, PFC PO2=95 mmHg) 140.0 Partial Pressure O2 (mmHg) 120.0 blood - capillary blood - tissue 100.0 80.0 60.0 40.0 20.0 0.0 0.000 0.020 0.040 0.060 Distance (cm) 0.080 0.100 Figure 5. Partial Pressure of Oxygen vs. distance along capillary( Blood and PFC 1:1, PFC PO2=145 mmHg) 0.120 120.0 100.0 blood - capillary Partial Pressure O2 (mmHg) 80.0 blood - tissue 60.0 40.0 20.0 0.0 0.000 0.020 0.040 0.060 0.080 0.100 0.120 -20.0 -40.0 Distance (cm) Figure 6. Partial Pressure of Oxygen vs. distance along capillary (Blood and PFC 1:1, PFC PO2=45 mmHg) References AP – Associated Press Release, Houston, 10 April 1998 Fournier, Ronald L. Basic Transport Phenomena in Biomedical Engineering. Philadelphia, PA: Taylor & Francis, 1995 Lawton, Graham. “Can Substitutes Solve the Blood Crisis?” Chemistry and Industry. 04 January, 1999: 9 Nucci, Mary L. and Abraham Abuchowski. “The Search for Blood Substitutes.” Scientific American. February 1998:72-77.