MRI Patient Questionnaire 8.24.15 (719)
advertisement
")
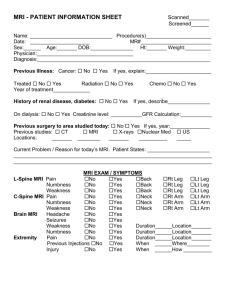
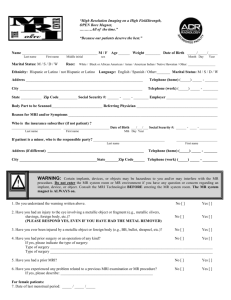
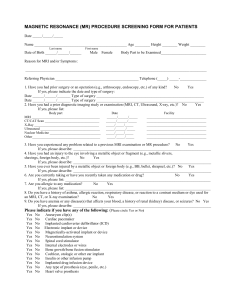
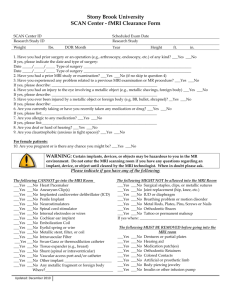
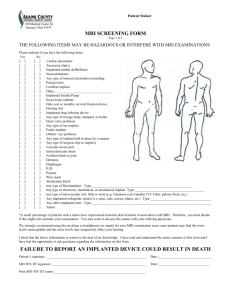
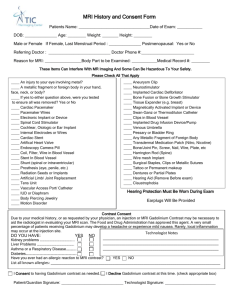
MRI Patient Questionnaire Patient Name: Date: Referring Provider: Date of Birth: Weight: Height: Personal History Cardiac Pacemaker – (circle one only please) Yes No If Yes, Medtronic Revo SureScan or Advisa DR MRI SureScan Bone growth/bone fusion stimulator Yes No Other implant Yes No Implanted cardioverter defibrillator (ICD) Yes No Any metallic fragment or foreign body Yes No Neurostimulation system Yes No Radiation seeds or implants Yes No Aneurysm clip(s) Yes No Internal electrodes or wires Yes No Tissue expander (e.g. breast) Yes No Heart valve prosthesis Yes No Cochlear, otologic, or other ear implants Yes No Joint replacement (e.g. hip, knee) Yes No Metallic stent, filter, or coil Yes No Wire mesh implant Yes No Shunt (spinal or intraventricular) Yes No IUD, diaphragm, or pessary Yes No Any type of prosthesis (eye, penile, etc.) Yes No Artificial or prosthetic limb Yes No Implanted drug infusion device Yes No Tattoo or permanent make-up Yes No Spinal cord stimulator Yes No Breathing problem or motion disorder Yes No Eyelid spring or wire Yes No Are you diabetic? Yes No Pill cam capsule endoscopy device Yes No Body piercing jewelry Yes No Surgical staples, clips, or metallic sutures Yes No Dentures or partial plates Yes No Medication patch (Nicotine, Nitroglycerine) Yes No Are you pregnant? Yes No Bone/joint pin, screw, nail, wire, plate, etc. Yes No Magnetically-activated implant or device; or electronic implant or device Yes No Swan-Ganz or thermodilution catheter or vascular access port and/or catheter Yes No Hearing aids (Remove before entering MRI system room) Yes No Injury to eye by metallic object: if yes – was it removed by a physician? ☐ Yes ☐ No Yes No IMPORTANT INSTRUCTIONS: Before entering the MR environment or MR system room, you must remove all metallic objects including hearing aids, dentures, partial plates, keys, beepers, cell phone, eyeglasses, hair pins, barrettes, jewelry, body piercing jewelry, watch, safety pins, paperclips, money clips, credit cards, bank cards, magnetic strip cards, coins, pens, pocket knife, nail clippers, tools, clothing with metal fasteners, & clothing with metallic threads. I attest that the above information is correct to the best of my knowledge. I have read and understand the contents of this form and have had the opportunity to ask questions regarding the MR procedure that I am about to undergo. Form Completed By: Signature: Relationship to Patient: Date: For Staff Use Only: Reviewed By: Staff: MRI Patient Questionnaire 8.24.15 Date: Staff: Date: (719) 785-9000 877-6-PENRAD • (877) 673-6723 PENRAD.org MRI Patient Questionnaire Patient Name: Date: Reason for examination? Are your symptoms related to an accident or injury? Yes No Date? Type of accident or injury: Is this exam a follow up to a prior injury or medical condition? Yes No (Specify):________________________ Have you had surgery on the body part(s) being scanned today? Yes No What procedure was performed? Date: Facility: Provider: Please list any other known medical conditions: Do you have a personal history of cancer? Yes No Where? What medications are you currently taking? Allergy or any reactions to MR contrast (Gadolinium) Yes No Are you allergic to any medications? Yes No Please list: Are you allergic to LATEX products? Yes No Circle Symptoms as they Apply to your Specific Exam Body MRI Difficulty Swallowing Yes No Nausea or Vomiting Yes Diarrhea Yes No Constipation Yes Jaundice (yellow skin) Yes No Pain Yes Brain MRI Headaches/Pain Yes No Seizures Yes Weakness Yes No Hearing Problems Yes Visual Problems Yes No Numbness Yes Speech Problems Yes No Difficult Walking Yes Difficult Thinking Yes No Eye MRI Which eye is involved? Right Left Both Is your vision affected? Yes No Blurred: Loss Of: Double Vision: Pain Yes No IACS or TMJ Ear Pain R L Ringing R L Deafness R L Pressure R L Hearing Loss R Teeth Pain R L Grinding R L Sensitivity R L Clicking R L Locking R Neck Pain R L Stiffness R L Musculosketal Pain Yes No Locking Yes No Swelling Yes No Infection Yes No Mass Yes No Spine MRI Pain Back Neck Right Leg Left Leg Right Arm Left Arm Weakness Back Neck Right Leg Left Leg Right Arm Left Arm Numbness Back Neck Right Leg Left Leg Right Arm Left Arm No No No No No No No L L Have you had previous radiology studies on the body part(s) being scanned today? MRI Location: MRI Location: CT Location: CT Location: UL Location: X-Ray Location: MRI Patient Questionnaire 8.24.15 (719) 785-9000 877-6-PENRAD • (877) 673-6723 PENRAD.org