NorthLake Medical Centre, PA
advertisement

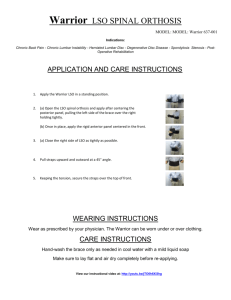
ABC Medical Billing Company 555 North Main Street Anytown, DE 01205 555-555-5555 Prescription, Pre-Auth & Medical Necessity Certification for LSO Brace – L0627, L0631, L0637 Patients Name: _____________________________________________________ DOB: _____________ ID #: _________________ Onset of DX’s: _____________________________________________________________________________________ Diagnosis: 1. ___________________________________ 3. _______________________________________ 2. ___________________________________ 4. _______________________________________ Diagnosis: ( ( ( ( ( ( ( ( ) ) ) ) ) ) ) ) 724.2 Low Back Pain ( ) 724.9 Nerve Root Compression 728.85 Muscle Spasm ( ) 722.10 Disc Displacement w/o myelo 728.9 Muscle Tightness ( ) 722.73 Disc Displacement w/ myelo 728.4 Ligamentous Instability ( ) 722.52 Lumbar Disc Degeneration 781.92 Abnormal Posture ( ) 847.2 Lumbar Sprain/Strain 737.10 Kyphosis ( ) 724.4 Lumbar neuritis/radiculitis 721.9 Spondylosis Other: _______________________________________________________________________ Relaxation of muscle spasm Absent Lumbar curvature causing pain Reverse Lumbar curvature causing pain Muscle re-education Expected Benefits (check all appropriate) Significantly reduce medication, as to frequency and amount Significantly increase mobility without pain Significant reduction of pain Improvement of postural/musculoskeletal abnormalities Duration of need: Prognosis: 12 Months Fair Reduction of neurological symptomatology Symptomatic relief and management of chronic pain Adjunctive treatment in the management of post- traumatic acute pain Improved clinical picture Avoidance of drug dependency Reduce exacerbations of disc injury Increase stabilization of Spine/SI joint Increase the stability of Spondylolesthesis Alternative Modalities Used: Stretching Electrical Stimulation Life Good Manual Therapies Intersegmental Traction PRN Pain (use indefinitely) Excellent Hot/Cold Therapies Neuromuscular Techniques Ultrasound/Iontophoresis Medicines previously tried dosage, duration and outcome. ____________________________________________________________________________________________________________ Instructions for use: Freq of use (___times per day); Length of use (___days, weeks, months); Time of Treatment (30 min, other___) _____The L0631, Lumbar-Sacral Orthosis, helps alleviate pain and speed rehabilitation by providing effective stabilization and unloading on the spine. It has sagittal control, with rigid anterior and posterior panels, posterior extends from sacrococcygeal junction to T-9 vertebra, produces intracavitary pressure to reduce load on the intervertebral discs, includes straps, closures, may include padding, shoulder straps, pendulous abdomen design, prefabricated, includes fitting and adjustment. _____The L0637, Lumbar-Sacral Orthosis, Sagittal Coronal Control helps alleviate pain and speed rehabilitation by providing effective stabilization and unloading on the spine. Lateral strength is provided by Rigid Lateral Frame/Panels. It has sagittal –coronal control, with rigid anterior and posterior panels, posterior extends from sacrococcygeal junction to T-9 vertebra, produces intracavitary pressure to reduce load on the intervertebral discs, includes straps, closures, may include padding, shoulder straps, pendulous abdomen design, prefabricated, includes fitting and adjustment. _____The L0627, Lumbar-Sacral Orthosis, helps alleviate pain and speed rehabilitation by providing effective stabilization and unloading on the spine. It has sagittal control, with rigid anterior and posterior panels, posterior extends from L1-L5 Vertebra. It produces intracavitary pressure to reduce load on the intervertebral discs, includes straps, closures, may include padding, shoulder straps, pendulous abdomen design, prefabricated, includes fitting and adjustment. Utilizing accepted medical practice standards the above-prescribed durable medical equipment is essential in the continuous treatment of this patient. Physician’s Signature: ________________________________________________ Date: _____ / _____ / ________ Physicians Name: __________________________________________________ Tax ID#: 45-1558702