Routine Deceased Donor Orders - Pediatric
advertisement

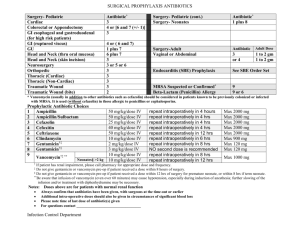
LifeShare Of The Carolinas Routine Deceased Donor Orders - Pediatric LifeShare Coordinator____________________________________ Blackberry # _____________________ DO NOT initiate these orders until patient is declared brain dead and consent obtained for donation Discontinue all previous orders except those specifically continued below Discharge patient and readmit as “Organ Donor” prior to entering new orders o Verify 2 hours of any necessary management drugs are available prior to discharging the patient o Attending Physician/Responsible Party: LifeShare Of The Carolinas Procedures: ______Arterial Line ______Triple or Quad Lumen Central Venous Catheter ______Swan Ganz ______Bronchoscopy – If available, please video record/photograph bronchoscopy Therapeutic and to assess for anatomical abnormalities Minimize lavage, avoid any unnecessary fluid Obtain current Weight:____________ kg Height:_______________ in Cardiology: _____Stat 12 lead EKG, NO Physician Interpretation Requested _____Stat Echo (Verify timing with LifeShare Coordinator prior to ordering) If available, provide electronic copy of echo images. Stat read and dictated report (including estimated LVEF %) required. Radiology: _____ AP Portable CXR* (evaluation and measurements for potential organ donation) Obtain lung measurement worksheet from LifeShare. Radiologist should complete and return. If central access placement is pending, wait until completed to order Laboratory: _____ Type* and crossmatch for 2 units PRBC’s CMV negative. Keep 2 units available at all times. Subgroup A blood types. Leuko-reduced, if available ALL LABS ARE STAT ORDERS _____ CBC* _____ CBC with Differential _____ CMP* _____ BMP* _____ Hepatic Function Panel* _____ PT/INR* _____ PTT* _____UA with Micro* _____ Phosphorous _____ Magnesium _____ Direct Bili* _____ Troponin I _____ Fibrinogen _____ Amylase/Lipase _____ HgbA1C Note to RN – DO NOT PERFORM POC TESTING UNLESS SPECIFICALLY REQUESTED OR ORDERED BY THE LIFESHARE COORDINATOR. _____Blood cultures* x 1 with sensitivity May obtain from Arterial and/or Central Venous Line if both/either are < 12 hours post insertion _____Urine culture* and sensitivity _____Bronchial washings for gram stain – to be obtained during bronchoscopy (order for potential lung donors only) 1 BAL sample from each lung (if initial gram stains are positive, perform bacterial culture only) 9/26/2010 Page 1 of 3 – Pediatric Verbal Order Medical Director and ____________________________________Date_____________Time___________ UNOS_______________ LifeShare Organ Recovery Coordinator Pharmacy: All medications are STAT orders _____Vasopressin: Mix 40 units in 250 ml NS; Dose= 0.5 milli-units/kg/hr May titrate at LifeShare’s direction to achieve desired urine output of __________ml/hr _____Artificial Tears or Normal Saline - 2 drops per eye every 2 hrs and tape lids closed Fluids: _____ Maintenance IVF_____________________, infused at_________ml/hr, add _________mEq KCl _____ Start urine replacement of______________, infused at ________ ml:ml/hr, add _______mEq KCl May titrate at LifeShare direction Vasopressors: (Notify LifeShare if max dose is exceeded or if a significant change in vasopressor requirements occurs) ______Dopamine infusion titrating dose from 1-20 mcg/kg/min ______Epinephrine infusion titrating dose from 0.1-1 mcg/kg/min ______Phenylephrine infusion titrating dose from 0.1-0.5 mcg/kg/min ______Vasopressors listed below to maintain a SBP of _____________: ______________________________________________________________________________________ ______________________________________________________________________________________ Antibiotics: ______Cefazolin (Ancef) 25mg/kg IV q 8 hrs (max: 1 gm/dose) ______Ceftazidime (Fortaz) 50mg/kg IV q 8 hrs (max: 2 gm/dose) ______Clindamycin (Cleocin) 10mg/kg IV q 6 hrs (max: 900 mg/dose) ______Ceftriaxone (Rocephin) 75 mg/kg IV daily ______Continue previous antibiotic coverage as follows – next dose due @ ______________________ ____________________________________________________________________________ ____________________________________________________________________________ Hormone Replacement Protocol: (Steroid, Insulin, Dextrose and Levothyroxine should be given in rapid succession) ______Methylprednisolone (SoluMedrol) ______30 mg/kg IV bolus (Total Dose=__________mgs) ______Repeat every 12 hrs ______Regular Insulin 0.1 units/kg IV (Total Dose=__________units) ______Dextrose ______D25 ______< 6 months of age 1-2mL/kg IV bolus x 1 (0.25-0.5 gm/kg/dose), max = 25gm/dose ______> 6 months to 12 years of age 2-4mL/kg IV bolus x 1 (0.5-1 gm/kg/dose), max = 25gm/dose ______D50 ______>12 years of age 50ml IV bolus x 1 (25 gm/dose) ______Levothyroxine: Mix 1000 mcg/50 ml NS (See chart below for dosing) Bolus should be administered over 30 minutes and then start infusion as indicated below: Check applicable Age Bolus (mcg/kg) Infusion (mcg/kg/hr) 0-6 months 5 1.4 6-12 months 4 1.3 1-5 years 3 1.2 6-12 years 2.5 1 12-16 years 1.5 0.8 9/26/2010 Page 2 of 3 – Pediatric Verbal Order Medical Director and ____________________________________Date_____________Time___________ UNOS_______________ LifeShare Organ Recovery Coordinator Respiratory: ______Initiate Ventilator Management Orders (see attached) _____Perform a Baseline ABG and an O2 Challenge at current ventilator settings (prior to Protocol initiation) _____Perform Baseline ABG prior to each O2 Challenge requested by LifeShare O2 Challenges to be performed as specifically directed in the Orders Verbally report all ABGs to LifeShare and document Tidal Volume, MAP, Plateau Pressure, and all other requested settings/parameters as directed on the LifeShare ABG Reporting Tool & Ventilator Worksheet. Follow guidelines on Orders for Ventilator Changes Additional Ventilator changes per LifeShare Chest PT and Rotation _____ HOB elevated 30 degrees _____Module rotation every 15 min. (side to side, never flat on back) _____Percussion 15 min every 2 hrs if not contraindicated _____IF NO MODULE AVAILABLE, Manual rotation (side to side, never flat on back) hourly _____Frequent pulmonary toilet Auscultate lung fields every 2 hrs. Notify LifeShare of any changes in breath sounds/secretions. Suction: Each time if chest PT produces secretions Every 4 hrs if nonproductive and clear breath sounds ______Do not initiate the Ventilator Management Orders. RT (in collaboration with LifeShare) to maintain/manage ventilator settings to optimize donor respiratory status. Maintain pH, PaCO2, and PaO2 within normal ranges, while minimizing FiO2. Verbally report ALL ABG results to LifeShare _____Perform Baseline ABG now _____Perform Baseline ABG every _____ hours _____Perform Baseline ABGs as directed by LifeShare Rotation, PT, auscultation of lung fields prn to maintain O2 saturation of 96% or better Nursing: _____ NG/OG tube to low continuous wall suction prn _____ Record VS every 15 minutes and CVP hourly Notify LifeShare Coordinator if: Heart Rate <__________ or > __________ beats/minute Systolic BP <__________ or >__________mmHg CVP <__________ or >__________mmHg Urine output < 1 ml/kg/hr or > 5ml/kg/hr O2 saturation < 96 % pH less than 7.35 _____ Blood Glucose checks every 1 hour Notify LifeShare Coordinator if > 150 mg/dL _____ Maintain patient temperature at 96.0 – 101.0 degrees Fahrenheit Use warming blanket and/or Baer Hugger as needed Record temperature hourly 9/26/2010 Page 3 of 3 – Pediatric Verbal Order Medical Director and ____________________________________Date_____________Time___________ UNOS_______________ LifeShare Organ Recovery Coordinator