Sacral Nerve Stimulation As Treatment of Neurogenic
advertisement

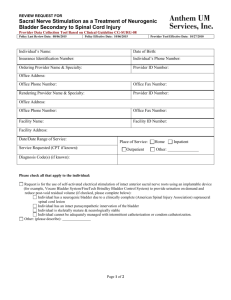
REVIEW REQUEST FOR Sacral Nerve Stimulation as a Treatment of Neurogenic Bladder Secondary to Spinal Cord Injury Provider Data Collection Tool Based on Medical Policy CG-SURG-08 Policy Last Review Date: 08/19/2010 Policy Effective Date: 10/13/2010 Provider Tool Effective Date: 03/28/2011 Individual’s Name: Date of Birth: Insurance Identification Number: Individual’s Phone Number: Ordering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Rendering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Facility Name: Facility ID Number: Facility Address: Date/Date Range of Service: Place of Service: Service Requested (CPT if known): Outpatient Home Inpatient Other: Diagnosis (ICD-9) if known): Please check all that apply to the individual: Request is for the use of self-activated electrical stimulation of intact anterior sacral nerve roots using an implantable device (e.g., Vocare Bladder System/FineTech Brindley Bladder Control System) to provide urination on demand and reduce postvoid residual volume (if checked, please complete below): Individual has a neurogenic bladder due to a clinically complete (American Spinal Injury Association) suprasacral spinal cord lesion Individual has an intact parasympathetic innervation of the bladder Individual is skeletally mature & neurologically stable Individual cannot be adequately managed with intermittent catheterization or condom catheterization. Other: (please describe): This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I attest the information provided is true and accurate to the best of my knowledge. I understand that Anthem may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. Page 1 of 2 REVIEW REQUEST FOR Sacral Nerve Stimulation as a Treatment of Neurogenic Bladder Secondary to Spinal Cord Injury Provider Data Collection Tool Based on Medical Policy CG-SURG-08 Policy Last Review Date: 08/19/2010 Policy Effective Date: 10/13/2010 Provider Tool Effective Date: 03/28/2011 _____________________________________________________________ Name and Title of Provider or Provider Representative Completing Form and Attestation (Please Print)* Date *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Page 2 of 2