Case study example
advertisement

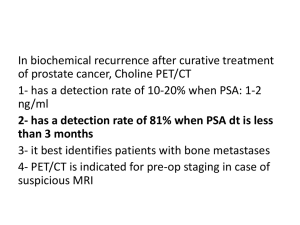
1. Describe a clinical scenario that you have recently encountered in approximately 200 words Finding a suitable clinical scenario can be a challenge. However on closer inspection there are questions that you could ask about the diagnosis, prognosis, aetiology and or treatment in the case of most patients that you encounter. In casualty you will be seeing patients at their pre diagnostic stage. Thus your questions may be about diagnosis, differential diagnosis, first steps in treatment, appropriateness of emergency management, positive and negative predictive values of symptoms and signs for certain diagnoses etc. If on the other hand you are working on a ward, the diagnosis has usually been agreed and you are looking at patients in which the most important issues are therapy, prognosis and causes (aetiology). Your questions may therefore be about choosing between therapeutic alternatives (why do we use this regime, is there an alternative? You may need to consider the evidence supporting one diagnosis as opposed to another etc. I have used a patient who presented in A/E at UCHG in early December recently to illustrate what I mean by an evidence based case report. The structure that I will use is the same one that I have given you on your instruction sheet. I hope that this gives you a good idea of what is expected of you. If you are still finding it difficult to find a suitable patient and/or choose a question etc. e-mail your questions to the department of medical informatics and medical education mime@nuigalway.ie . I am happy to help you to choose patients, frame questions and to give you some advice on searching The case that I chose was the following: A 55 year old man was sent to casualty by his GP complaining of vague back pain. The GP’s letter stated that the man had suffered from urinary hesitancy, dribbling, double voiding etc. for some time. His Prostate Specific Antigen was 46 and he had evidence of possible sclerotic lesions on a spinal x-ray. The GP concluded that man had probable prostatic cancer with spinal metastases. The patient was seen by the urology registrar who agreed with the probable diagnoses. He ordered a bone scan, a repeat PSA test and renal function tests. I wondered whether a prostate specific antigen of 46 was predictive enough of metastatic spread. Was an expensive bone scan really necessary? (114 Words) 1. From this scenario create a structured question for which you require an “evidence based” answer To create a structured question you will need to identify what are the questions that you want to look into about this patient’s case. Of these questions which is the most pertinent, interesting etc.? Once you have decided which question you want to use you then need to put that question into a form that will allow you to find some answers. The best method is to try to put the question into a structure that resembles the following: The patient or problem The intervention or therapy or prognostic factor or cause A comparison intervention or cause (if there is one?) An outcome that you want to know about Here are some examples Patient or problem Intervention, cause, prognostic factor etc. Comparison intervention Outcome Starting with your patient ask “how would I describe a group of patients similar to mine. Which intervention, cause etc. am I considering? What is the main alternative? What do I/ we hope to accomplish? In patients who have atrial fibrillation and a dilated left ventricle on ECHO Does anticoagulation with warfarin Compared with standard A Fib. Therapy alone Reduce the rate of thromboembolic events e.g. stokes Diagnosis question In patients who present with symptoms and signs suggestive of appendicitis Does a raised neutrophil count on an FBC test Compared to a normal neutrophil count Increase the likelihood that the patient has appendicitis Prognosis question In patients undergoing lower limb arterial bypass surgery Does a history of previous myocardial Infarct Compared to patients no with no evidence of a previous MI Lead to a longer recovery period or greater incidence of post-operative complications etc.? Tips: from Sackett et al. See book reference at the end of this case report Therapy question My structured question is as follows: In patients with suspected metastatic prostate cancer in whom the PSA is >20mcg/L does the addition of radionucleotide bone scanning, compared with PSA screening alone make a significant difference to the detection of metastatic prostate cancer. The key words that I thought might be useful for this search question are: prostate specific antigen, radionucleotide bone scan, predictive value of tests, diagnosis, I tried a quick Medline search using these terms. I found one article that covered the topic of PSA and Bone Scans. I looked at the “Complete Reference” for the paper. It included a list of all the MeSH terms used to code the article. I used some of these terms to add to my search term list: Prostate-specific antigen/bl (blood test = bl) Prostate neoplasms/bl Prostate neoplasms/ri (radionucleotide investigation) Predictive value of tests Prognosis Neoplasm staging/mt (metastatic) I have put together a useful Internet search list for you. These sites include Search engines, Databases, on-line journals etc. I strongly recommend that you use Doctors Desk as a starting point as it links to many on-line journals, the Cochrane Database, free Medline and Bandolier. The list is available on the Q Drive and is labelled EBM Toolbox 2. Study the abstracts of the studies that you have found and identify 5 key papers that answer your question. Please ensure that these papers are either available in full text on-line or that the relevant journal is held by the Hardiman library. You will be required to submit the 5 full text papers with your completed evidence based case study. A list of all the journals held by the Hardiman library can be found on the library website. The five papers used in this evidence based case report a) b) c) d) e) PSA and Bone Scans, Bandolier Vol.47 No. 4 Serum PSA predicts negative Bone Scan Bandolier Vol.2 No.4 Haukaas S., Roervik J., Halvorsen OJ, Foelling M. When is bone scintigraphy necessary in the assessment of newly diagnosed untreated prostate cancer; British Journal of Urology. Vol.79 (5):770-6, 1997 The positive yield of imaging studies in the evaluation of men with newly diagnosed prostate cancer: a population based analysis. Albertsen PC; Hanley JA; Gilliland FD; Hamilton A; Liff JM; Stanford JL; Stephenson RA. The Journal of Urology Vol. 163 (4): 1138-43 Lin K; Szabo Z; Chin BB; Civelek AC; The value of a baseline bone scan in patients with newly diagnosed prostate cancer. Clin Nuc Med Vol. 24 (8): 579-82. 3. Give a brief description of each paper in terms of its study design methodology relevance to your question quality Paper 1: PSA and Bone Scans Study design This is a review of a paper published in the British Journal Of Urology Methodology The paper summarises the findings from the original paper Relevance to your question This paper is included because it provides useful evidence supporting the avoidance of bone scans in patients who have PSA levels < 20mcg/L Quality The paper is well presented, brief and accurately reports the findings of the original paper Paper 2: Serum PSA predicts negative Bone Scan Study design This is a report of a paper published in The Journal Of Urology Methodology The paper summarises the findings from the original paper Relevance to your question This paper is included because it provides a detailed description of the original study findings. It explains that bone scans are expensive and unpleasant. PSA alone is 99.7% predictive of the presence of Bone metastases in prostatic cancer. The paper argues strongly for the abandonment of bone scans in patients who’s PSA is <20 Quality The paper is well presented, and reports the findings from an original paper. It is important to check the original paper for any factual inaccuracies or potential misinterpretations Paper 3: When is bone scintigraphy necessary in the assessment of newly diagnosed untreated prostate cancer Study design Cross sectional survey of 128 patients newly diagnosed with prostate cancer comparing the prevalence of bone metastases at different levels of PSA. Methodology The authors measured PSA in men with newly diagnosed cancer. They then did a bone scan on each patient. The correlated the bone scan findings with the PSA scores. The authors then estimated the positive predictive value of PSA for bone metastases at different values of PSA Relevance to your question This paper is included because it provides evidence that a PSA of < 20 is predictive of the absence of bony metastases. Quality The study is well constructed, it has a small but reasonable number of subjects and there are no obvious biasing factors Paper 4: The positive yield of imaging studies in the evaluation of men with newly diagnosed prostate cancer: a population based analysis. Study design Prospective survey of 3,690 patients newly diagnosed with prostate cancer comparing the prevalence of bone metastases on Bone scan and CT scan at different levels of PSA. Methodology The clinics involved in the study measured PSA in men with newly diagnosed cancer. They then did a bone scan, a CT scan and in some cases and MRI on each patient. The correlated the bone scan findings with the PSA scores. The authors then estimated the positive yield of PSA in identifying bone metastases at different values of PSA. Relevance to your question This paper is included because once again it provides evidence that a PSA of < 20 is predictive of the absence of bony metastases. Quality The study is reasonably well constructed. It has a large number of subjects and there are no obvious biasing factors. One weakness is that the authors do not calculate a positive predictive value for the PSA but express their results in terms of the correlation between PSA value and positive bone scans. This is not as immediately useful a result as predictive value. Paper 5: The value of a baseline bone scan in patients with newly diagnosed prostate cancer. Study design Retrospective survey of the records of 270 patients with newly diagnosed with prostate cancer Methodology The authors analysed the records of 270 men who had been diagnosed with Prostate Cancer between 1995 and 1997. They correlated positive bone scans with PSA measurements Relevance to your question This paper is included because it provides evidence that a PSA of < 10 is predictive of the absence of bony metastases. The implication of the paper is that metastatic spread might be missed in a few cases if the PSA threshold was set at 20 Quality The study is retrospective and is therefore open to record inaccuracies. The authors did not explain whether the group of 270 was a sample taken from a larger population or constituted all the patients attending one centre. Nonetheless the results seem credible and could influence the PSA threshold that is chosen for deciding about a bone scan. 4. Synthesise the findings from the 5 papers into an answer to the clinical question that you set for yourself. (Answers should be between 1000 and 2000 words long). Include a paragraph of your conclusions. The question that I set for myself has turned out to be a two stemmed query. The first question is whether a PSA of 46 means that metastatic disease is certain and a bone scan is unnecessary to confirm it. The second question is whether it is safe not to do a bone scan in patients with a PSA of < 20. From these 5 papers I can say that the PSA is better at ruling out (negative predictive value) disseminated prostatic cancer than it is at diagnosing prostatic metastatic disease1 If the PSA is < 10 the likelihood of having disseminated cancer is < 0.5% 2 If the PSA is < 20 the likelihood of having disseminated cancer rises to between 0.1 and 1.8%3 Thus it would be safe to base a decision not to scan on the basis of a low PSA result (particularly if , < 10mcg/L)4,5. It is conversely not safe to assume that a PSA result > 20 implies that metastasis has taken place. 5. List the references to your 5 key papers in the order in which you refer to them in the text of your case study using the Vancouver style 1. PSA and Bone Scans, Bandolier Vol.47 No. 4 2. Serum PSA predicts negative Bone Scan Bandolier Vol.2 No.4 3. Haukaas S; Roervik J; Halvorsen OJ; Foelling M. When is bone scintigraphy necessary in the assessment of newly diagnosed untreated prostate cancer. British Journal of Urology. Vol.79 (5):770-6, 1997 4. Albertsen PC; Hanley JA; Gilliland FD; Hamilton A; Liff JM; Stanford JL; Stephenson RA The positive yield of imaging studies in the evaluation of men with newly diagnosed prostate cancer: a population based analysis. The Journal of Urology Vol. 163 (4): 1138-43 5. Lin K; Szabo Z; Chin BB; Civelek AC; The value of a baseline bone scan in patients with newly diagnosed prostate cancer. Clin Nuc Med Vol. 24 (8): 579-82. 6. Submit your completed case study with copies of the 5 papers used as evidence to Dr Cantillon at the Department of Medical Informatics and Medical Education on or before the 28th of February 2001 Word count including references and excluding instructions is 1309