risks distal
advertisement

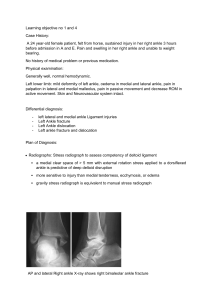
BRIEF HISTORY: The patient is a 77-year-old retired gentleman who complains of right ankle pain that started on January 4, 2009 when he slipped on some black ice and twisted his ankle. He was seen by Dr. Eakin and was found to have a distal fibula fracture and a widened mortise. He was placed into an above-the-knee condylar cast for 2 weeks, and then subsequently into a Cam walker boot. He has remained nonweightbearing for the last 3 weeks. He has noticed continued pain. Overall, he thinks things are staying the same. His pain is better with rest and worse with motion. He has no radiation of his symptoms. No numbness. He is currently taking occasional Vicodin for his pain. He does have a history of diabetes but denies any history of retinopathy, nephropathy, neuropathy, or coronary artery disease. On a scale of 1 to 10, he rates his pain as 7 out of 10. He typically is not participating in any regular exercise program. He typically wears tennis shoes, and prior to his injury his walking tolerance was unlimited. PHYSICAL EXAMINATION: GENERAL: The patient is generally well appearing, in no acute distress. Stated height and weight is 5 foot 6 inches, 160 pounds. HEENT: Normocephalic, atraumatic. Oropharynx is clear HEART: Regular rate and rhythm. LUNGS: Unlabored respirations. ABDOMEN: Nontender, nondistended. RIGHT LOWER EXTREMITY: He has a neutral lower extremity alignment. He has an antalgic right gait. He has tenderness to palpation particularly along the distal fibula and ATFL. He has less tenderness medially, though he is somewhat tender along his medial gutter. He has mild diffuse swelling of his ankle. His skin is intact. His sensation is intact to monofilament testing. His ankle motion and stability are guarded. IMAGING: X-rays reveal a distal fibular fracture with medial mortise widening. ASSESSMENT AND PLAN: Right ankle distal fibula fracture with widened mortise. Discussed the nature of this problem with the patient and discussed both conservative and surgical treatment options. We have discussed with him that if treated conservatively he has a higher risk going on to develop ankle arthritis down the road. We would recommend at this point a surgical fixation, though this does carry some risk of wound healing problems related to his diabetes, and infection. At this point, we feel that the risk is lower than not operating. We discussed with him further the risks, benefits, and alternatives which include but are not limited to damaging nerve, tendons, or blood vessels, bleeding, wound healing problems, infection, stiffness, need for further physical therapy, continued pain, or down the road even the chance of developing arthritis. He understands these risks and wishes to proceed. arrange this for him. We will help to Dr. Haskell was present for the history and physical examination of this patient.