Patient Medical History
advertisement

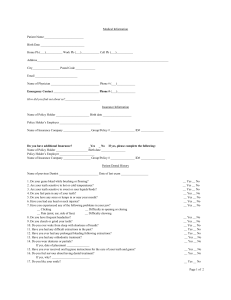
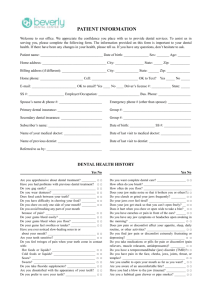
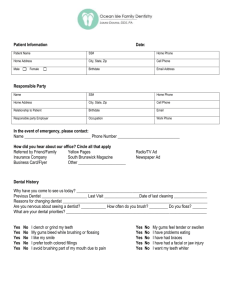
Patient Medical History PHYSICIAN: Date: OFFICE PHONE: LAST EXAM DATE: Are you taking any medication, including non-prescription medicine? If yes, list the medications here: Yes □ No □ Have you been hospitalized for any surgical operation or serious illness in the last 5 years: If yes, explain: Yes □ No □ Are you allergic or have you had any reactions to the following? Yes □ Yes □ Yes □ Yes □ Yes □ Local Anesthetics (e.g. Novocain) Penicillin or other antibiotics Sulfa Drugs Barbiturates Any Metals (nickel, mercury, etc) Do you use tobacco? Do you use controlled substances? Women: Yes □ No □ Yes □ No □ No □ No □ No □ No □ No □ Sedatives Iodine Aspirin Latex Rubber Other Do you wear contacts? Are you pregnant or do you think you are pregnant? Are you taking oral contraceptives? Are you nursing? Yes □ Yes □ Yes □ Yes □ Yes □ No □ No □ No □ No □ No □ Yes □ No □ Yes □ No □ Yes □ No □ Yes □ No □ Please circle any of the following conditions that you have, or have had in the past: High Blood Pressure Low Blood Pressure Heart Trouble Heart Disease Stroke Heart Attack Cardiac Pace Maker Angina Fainting/Seizures Persistent Diarrhea S. T. D. Chest Pains Heart Murmur Mitral Valve Prolapse Easily Winded Hay Fever/Allergies Asthma Respiratory Problems Rheumatic Fever Hemophilia Frequently Tired AIDS or HIV Joint Replacement /Implant Emphysema Cancer Leukemia Radiation Therapy Kidney Disease Liver Disease Diabetes Hepatitis/Jaundice Recurrent Fevers Other: Thyroid Problem Anemia Arthritis Glaucoma Tuberculosis Epilepsy/Convulsions Swollen Ankles Stomach Troubles/Ulcers Recent Weight Loss Chills/Night Sweats Dental History NAME OF PREVIOUS DENTIST: DATE OF LAST EXAM: Do your gums bleed while brushing/flossing? Yes □ No □ Do you have frequent headaches? Yes □ Are your teeth sensitive to hot or cold? Yes □ No □ Do you clench or grind your teeth? Yes □ Are your teeth sensitive to sweet or sour? Yes □ No □ Do you bite your lips or cheeks? Yes □ Have you injured your head, neck, or jaw? Yes □ No □ Have you had orthodontic treatment? Yes □ Do you wear dentures or partials? Yes □ No □ Placement date: Do you have any sores or lumps near or around your mouth? Yes □ Have you ever had any prolonged bleeding following extractions? Yes □ Have you ever received oral hygiene instructions regarding the care of your teeth and gums? Yes □ Have you ever experienced any of the problems with your jaw? Please circle all that apply. Clicking Pain (joint, ear, side of face) Difficulty opening or closing Difficulty chewing Do you like your smile ☺ ? No □ No □ No □ No □ No □ No □ No □ Yes □ No □ If no, explain: I have truthfully answered all the above questions and agree to inform this office of any changes in my medical or dental history. Patient Signature or Responsible Party Signature if patient is a minor Date