View the supporting material
advertisement

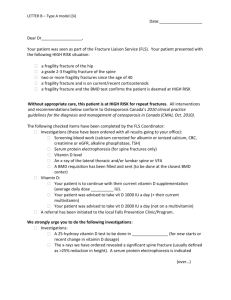
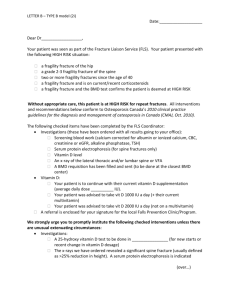
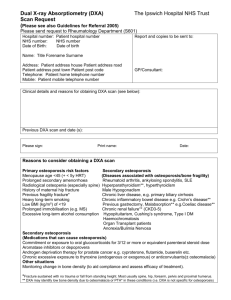
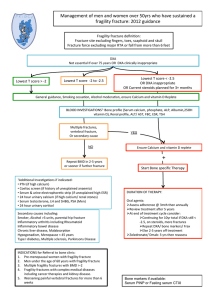
Dear Doctor The above named patient has recently attended fracture clinic in the trauma and orthopaedic department at Morriston Hospital due to a low trauma fracture. This fracture makes them at high risk of osteoporosis. 1. The patient is under 75 years of age or male and has therefore been referred for a DXA scan at Singleton Hospital. The results of the scan when performed will be sent to you, for further treatment Any male patients with a confirmed diagnosis of osteoporosis and currently not receiving any oral steroid treatment should then be referred to the Bone clinic at Hill House Hospital under Dr. Harris for further management. Please could you arrange this if diagnosis is confirmed? 2. The patient is 75 years or above and a DXA scan is considered clinically inappropriate or unfeasible. We recommend that the patient be started upon treatment as per the treatment protocol on the reverse based upon the current NICE guidelines 3. The patient is currently taking oral steroids and therefore has had a DXA scan requested. The patient should be treated for osteoporosis with a bone score of T< 1.5S>D ( not 2.5) 4. The patient has already had a diagnosis of osteoporosis and has been taking bone sparing treatment for > 1 year and therefore requires referral to the bone clinic at Hill House Hospital under Dr. Harris 5. The patient has been on treatment of osteoporosis for < 1 year. We ask that you monitor their persistence with therapy and arrange a repeat DXA scan in 18 months 6. The patient has a previous diagnosis of osteoporosis but is currently not taking any bone sparring therapy and therefore needs a medication review in accordance with the enclosed guidelines Thank you Trauma and Orthopaedic Department Morriston Hospital TREATMENT GUIDELINES FOR THE SECONDARY PREVENTION OF OSTEOPOROTIC FRAGILITY FRACTURE IN POSTMENOPAUSAL WOMEN* This guideline relates only to treatment for the secondary prevention of fragility fractures in postmenopausal women who have osteoporosis and have sustained a clinically apparent osteoporotic fragility fracture. It does not take into account treatments for primary prevention. It should be ensured that patients have adequate calcium intake and are vitamin D replete. If this cannot be assured then calcium and vitamin D should be prescribed as Adcal D3 one twice a day. N.B Prior to treatment patient’s eGFR must be checked to be >30 and their serum calcium checked. Which Treatment? 1. Generic alendronate 70mg once a week is recommended as first line treatment when osteoporosis has been confirmed (that is, T-score of –2.5SD or below). 2. Risedronate 35mg once a week can be used as alternative treatments only when the patient is unable to comply with the administration instructions for alendronate or have contraindication or intolerance1 to it. 3. Strontium ranelate and raloxifene can be used only when the patient is unable to comply the administration instructions for the alendronate and either risedronate or have contraindication or intolerance to alendronate1 and either risedronate1 or etidronate1 . If a woman aged 75 years or older who has one or more independent clinical risk factors for fracture or indicators of low BMD has not previously had her BMD measured, a DXA scan may not be required if the responsible clinician considers it to be clinically inappropriate or unfeasible. If intolerance to all above treatments then the patient requires referral to the bone clinic at Hill House Hospital for further management. 1. Intolerance of alendronate, risedronate or etidronate is defined as persistent upper gastrointestinal disturbance that is sufficiently severe to warrant discontinuation of treatment, and that occurs even though the instructions for administration have been followed correctly. 2. Intolerance of Strontium ranelate is defined as persistent nausea or diarrhoea, either of which warrants discontinuation of treatment. 3. An unsatisfactory response is defined as occurring when a woman has another fragility fracture despite adhering fully to treatment for one year and there is evidence of a decline in BMD below her pre-treatment baseline. Women who are currently receiving treatment with one of the drugs covered in this guidance, but for whom treatment would not have been recommended according to sections 1-4, should have the option to continue treatment until they and their clinicians consider it appropriate to stop. * Adapted from NICE technology appraisal guidance 161.