SUMMARY OF CLINICAL ANATOMY OF HEAD AND NECK
advertisement

SUMMARY OF CLINICAL ANATOMY OF HEAD AND NECK - parts A and B
© 2010zillmusom
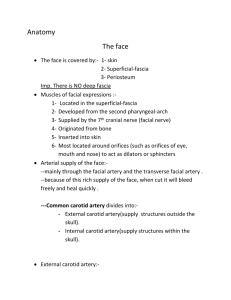
Clinical
Anatomy
Cause
Anterior Cranial Fossa - Cranial nerve I, Nasal Cavity
Fracture of
Nasal septum continuous
Blow to nose;
cribriform plate of
with crista galli of ethmoid
fracture produces
ethmoid bone
bone; Olfactory nerve
continuity
passes through cribriform
between
plate of ethmoid bone
subarachnoid
space and nasal
cavity
Middle Cranial Fossa - Cranial nerves II-VI Orbit, Eye Movements, Face
Rapid loss of vision Central artery of retina
Occlusion of
in one eye
(branch of Ophthalmic
central artery of
artery from Int. Carotid) is
retina
an end artery with no
functional anastomoses
Slow loss of vision
Dura mater and
Communicating
in one eye
subarachnoid continue over hydrocephalus
optic nerve; nerve function (many causes)
can be affected by CSF
pressure
Abducens nerve
palsy
Abducens nerve innervates
only Lateral Rectus muscle
(action: abduction of eye)
Trochlear nerve
palsy
Trochlear nerve innervates
only Superior Oblique
muscle (action: abduct,
depress and medially rotate
eye)
Oculomotor nerve
innervates Superior, Medial
and Inferior Rectus and
Inferior Oblique; part of
Levator palpebrae
superioris; also provides
parasympathetics to
pupillary constrictor, ciliary
muscles
Sympathetics in head
innervate smooth muscle
part of Levator Palpebrae
Oculomotor nerve
palsy
Horner's Syndrome
Damage
Abducens nerve
VI (causes ex.
increased
intracranial
pressure,
Cavernous sinus
thrombosis)
Damage
Trochlear nerve
(ex. trauma)
Damage
Oculomotor nerve
(frequently
idiopathic)
Block conduction
in Sympathetics
to head (tumors,
Sign/Symptom
Leakage of CSF from
nose ('runny nose')
Sudden onset
blindness in one eye
(one eye only, artery
visible through
ophthalmoscope)
Decreased visual
function both eyes
(diagnose as
papilledema in
ophthalmoscope);
also other signs
increased intracranial
pressure (headache,
etc.)
Diplopia and Medial
strabismus
Inability to look down
and out (difficulty
walking down stairs);
Head tilted toward
side opposite lesion
Lateral strabismus,
dilated pupil, ptosis;
also loss of
accommodation
(near vision) due to
paralysis of ciliary
muscles
Ptosis (drooping
eyelid from smooth
muscle part of
Superioris; Pupillary dilator etc)
Levator Palpebrae
muscle; sweat glands of
Superioris);
skin; Pathway: preConstricted pupil
ganglionic Sympathetics
(miosis due to
arise at T1,2; ascend in
paralyze Dilator
chain; post-ganglionics in
pupillae); Anhydrosis
Sup. Cerv. Ganglion;
of forehead
distributed with arterial
(denervate sweat
branches (Ophthalmic
glands)
artery)
Cavernous sinus
Branches of cranial nerves Infection of face
Diplopia (blurred
thrombosis
(III, IV, V1, V2, VI) and
at angle of nose
vision) due to
Internal carotid artery pass
or upper lip
disruption of eye
through wall of cavernous
particularly
movements;
sinus; Cavernous sinus
dangerous
increased venous
drains ophthalmic veins
pressure produces
which anastomose with
engorgement in veins
branches of Facial Vein;
of retina
veins have no valves
Epidural Hematoma Middle Meningeal artery
Blow to side of
Patient conscious
(branch of first part of
head (region of
after accident; loses
Maxillary artery that passes pterion)
consciousness with
through foramen spinosum)
hours; coma death
supplies bone of calvarium
Subdural
Bridging veins link
Blow to head; in
Slow onset of
Hematoma
Superficial cerebral veins
elderly can occur neurological
on surface of brain and
without distinct
symptoms, headache
Superior Sagittal sinus
event
(often hours to days)
(also other venous sinuses)
Communicating
CSF produce in choroid
Calcification of
Head ache,
Hydrocephalus due plexus; reabsorbed from
arachnoid villi
papilledema
to decreased CSF
subarachnoid space at
(arachnoid
reabsorption (in
arachnoid villi into venous
granulations)
elderly)
sinuses
Numbness of
V is major sensory nerve of Many; ex.
Numbness in specific
regions of face
face and head; V1 above
Trigeminal
region can be
lateral margin eyelids; V2
Anesthesia
correlated with
eyelids to upper lip; V3
specific division of V
below lateral margins of lips
Pain in external
Skin of ear and external
Bell's palsy
Ear ache (following
auditory meatus
auditory meatus gets
or accompanying
following Facial
sensory innervation from
Facial paralysis)
paralysis
V, VII, IX and X
Weakness of
Muscles mastication
ex. Tumor at
When open mouth,
muscles mastication innervated by V3; Lateral
foramen ovale
jaw deviates toward
Pterygoid opens mouth; all
paralyzed side
other muscles Mastication
close mouth
Posterior Cranial Fossa - Cranial Nerves VII-XII, face, ear, pharynx, tongue
Facial paralysis
CN VII and VIII exit post.
Acoustic neuroma Loss or reduction of
(with effect on VIII)
Facial paralysis (no
effect on VIII)
Loss of function of
IX and X
Hoarse voice after
thyroid surgery
Torticollis
Paralysis of
muscles of tongue
cranial fossa via Internal
auditory meatus; VIII ends
in temporal bone; VII enters
facial canal and gives off
branches in temporal bone;
1) parasymp. to Lacrimal
gland, mucous glands of
nose, palate; 2) Nerve to
Stapedius muscle; 3)
Chorda tympani - taste to
ant. 2/3 of tongue;
parasymp. to
Submandibular, Sublingual
salivary glands
Facial nerve exits skull via
Stylomastoid foramen; only
has motor branches after
leaving skull
Parotid tumor
IX is major sensory nerve
to pharynx (oropharynx);
X is motor to all muscles of
pharynx except
Stylopharyngeus; all
muscles of palate (except
Tensor palati)
X is motor to all muscles of
larynx; also sensory to
larynx; Recurrent Laryngeal
nerve passes posterior to
Thyroid gland with Inf.
Thyroid artery; is motor to
all laryngeal muscles
except Cricothyroid
XI innervates
Sternocleidomastoid and
Trapezius
Tumor at Jugular
Foramen
XII is motor to all muscles
of tongue (no sensory
component)
XII hypoglossal
nerve palsy
hearing in one ear;
Full Facial nerve
palsy (Bell's palsy)
symptoms:
1) Facial paralysis
and loss of Corneal
reflex (V1 sensory,
VII motor)
2) loss of taste to ant.
2/3 of tongue,
3) decreased
secretion tears and
saliva
4) Hyperacousia
Facial paralysis; Loss
of corneal reflex but
no loss of taste or
decrease in tears or
saliva; no
hypercousia
Difficulty in
swallowing; Absence
of gag reflex; (Gag
reflex - IX sensory, X
motor)
Damage
Recurrent
Laryngeal nerve
during Thyroid
surgery
Hoarse voice due to
unilateral paralysis of
all laryngeal muscles
(except Cricothyroid)
Torticollis can be
congenital or
acquired
Contracture of
Sternocleidomastoid
- head is rotated with
face directed to
opposite side
Atrophy of muscles of
tongue on one side;
protruded tongue
deviates toward side
of lesion due to
Genioglossus)