MRI Screening Form - Waisman Laboratory for Brain Imaging and
advertisement

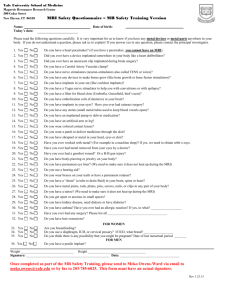
MRI Screening Form Key ___________________________________________________________________________________________________________ Date: _____/_____/_____ By: ___________________________________ Subject: ____________________________________________________________________________ Study: _________________________ PI: ___________________________________ ID#: ___________________________ SS#: _____-_____-_____ Sex: Female Age: ______ Male DOB: _____/_____/_____ Weight: _______ Home Phone: _____-_____-_____ Height: ____’____” Work Phone: _____-_____-_____ Hat Size: ______ Recruitment: ____________________________ This is a tricky issue, and persons having heads too large to fit into the head coil (with goggles and bite bar) are actually rather common. The critical dimension is not really hat size, per se, but rather the dimension from the occiput to the front of the mouth. The reason for asking about hat size is really rule-of-thumb. Persons reporting hat sizes greater than 7 ¾ will probably not fit in the head coil. This issue is furhter complicated by the fact that very few people know their hat size. ___________________________________________________________________________________________________________ General rule: We are doing research, not medical diagnosis. Our subjects don’t need the MRI for diagnosis of a medical problem. Because of that, we should be very conservative in our acceptance of subjects. If an item come up that leads you to reject a subject, explain the importance of these screening procedures and the fact that we are being particularly strict because this is controlled research and not necessary diagnosis. With a patient population, this will require delicate wording. Yes ___ No ___ ___ ___ ___ ___ ___ ___ Do you have corrected vision? Do you know your vision rating or prescription?_______________________________________________ ___ ___ Do you wear contact lens? The reason for asking these questions relates to the goggles that will be used to present visual stimuli. We don’t really know the range of vision that we can accommodate with the focus on the device. If subjects can wear contacts, they should. If someone reported vision of something extreme, say 2000/2000, I would question their compatibility. This is really a rule-of-thumb issue. Do you have TMJ (Temporal Mandibular Joint) disorder or other problems with biting/chewing? Type? _________________________________________________________________________________ This has to do with the Bite Bar. We don’t know what problems might occur with this, but because they will have the device in their mouth in a stationary position for over one hour, we should be sensitive to potential problems. I don’t know how often this issues will come up, but I would describe the Bite Bar and see what the subject’s reaction is. If some one is positive for TMJ, I would not accept them. There have been complaints of pain from subjects who had TMJ and we didn’t know it. Have you ever had an MRI scan? When? ________________________________________________________________________________ Why? _________________________________________________________________________________ This is background. If they have had an MRI, they were once safe, but that does not mean that are still safe If they had an MRI for some type of head injury, for example a car accident, that may alert to potential problems that the questions below will not specifically address. Have you ever had surgery? When? ________________________________________________________________________________ Type? _________________________________________________________________________________ Surgery involves metal parts entering the body. Often times this results in intentional placement of metal in the body (i.e., clips or screws), and, in rare cases, metal can be left in the body accidentally. If there has been a surgery, inquire about the type, are stitches MR Screening, Key, Rev 03/07/01, WI, Page 1 still present, were staples used to close any openings, etc. The questions will be motivated by the type of surgery. Recent surgery would not exclude a subject, but we want to know if there are potential problems. ___ ___ Have you ever had heart surgery? When? ________________________________________________________________________________ Type? _________________________________________________________________________________ If someone has had heart surgery, there is the chance that something was implanted. Cardiac pace wires (of which the subject may not even be aware) can remain. At this point, I would not accept anyone who has had heart surgery. ___ ___ Do you have a Pacemaker? ___ ___ Do you have an implanted cardiac defibrillator? ___ ___ Do you have an artificial heart valve? ___ ___ Do you have cardiac pace wires? ___ ___ Have you ever had head or brain surgery? Unless this was the focus of the study, for both scientific and saftey reasons, I would not accept anyone who has had brain surgery. They are, by definition, not of the same category as non-brain surgery subjects. When? ________________________________________________________________________________ Type? _________________________________________________________________________________ ___ ___ Have you ever had eye surgery? ___ ___ Do you have lens implants? Lens implants should be a flag. While not metal, they could affect the tissue heating that is a result of the physics of MRI. I would reject subjects with lens implants. Cataract surgery done before 1986 (or thereabouts) needs to be followed up. ___ ___ Do you wear dentures? Many dentrues have metal in their design. The subject might be required to remove them for the scan. Some type of dental implants are actually held in place with magnets. ___ ___ Have you ever had ear surgery? ___ ___ Do you have a cochlear implant? ___ ___ Do you wear a hearing aid? Reject subjects with ear implants. If the subject wears a hearing aid, highlight this item so that at the time of scan it is removed. ___ ___ Have you ever had back surgery? When? ________________________________________________________________________________ Type? _________________________________________________________________________________ This is a warning indicator. Persons with back trouble (past or current) may not be able to be supine for the duration of the scan. ___ ___ Do you have any implanted devices of any type? ___ ___ Breast/Penile? ___ ___ Electrodes? ___ ___ Pumps (e.g., drug infusion device)? ___ ___ Bone or socket? ___ ___ Neurostimulators/Biostimulator? Reject subjects with these types of implants. Some bone & socket replacements may be acceptable. ___ ___ Do you have any dental or orthodontic implants (fillings are O.K.)? Type? _________________________________________________________________________________ Braces are not acceptable. Most types of permanent retainers are acceptable (i.e., those that stabilize the front teeth). ___ ___ ___ ___ ___ ___ ___ ___ Do you have any type of prosthesis? Type? _________________________________________________________________________________ Mechanical prostheses would need to be removed. Do you have any type of orthopedic implant (e.g., pins, rods, screws, nails)? Type? _________________________________________________________________________________ This is a warning indicator. Depending on location and material, they may be acceptable. Do you have any permanent cosmetics (e.g., eyeliner)? Do you have any tattoos on your upper body? Where/Extent? _________________________________________________________________________ MR Screening, Key, Rev 03/07/01, WI, Page 2 The ink used in tattoos and permanent cosmetics can have a metallic base and can cause “tissue heating” in some cases. This is not necessarily a rejection factor, but we should know about it. ___ ___ Do you have any body piercing(s)? Where? ________________________________________________________________________________ Any earrings on the head must be removed. Piercings on other parts of the body may have to be removed. ___ ___ Do you have a history of any metal in your body? Obviously we need to know about this. Rejection depends on the what, where & how. ___ ___ Have you every worked as an occupational metal grinder? Description: __________________________________________________________________________ Working with metal often leads to accidents in which metal gets into and remains in the body. ___ ___ Have you ever worked with metal as a hobby? Description: __________________________________________________________________________ ___ ___ Did you routinely wear safety glasses? Many people answer “yes” to the hobby question. For example, “sharpening ice skates.” It is very important that you pursue this to inquire exactly what they did and for how long. It is essential that they tell you they wore safety glasses. ___ ___ Have you ever sought medical attention for metal in your eyes? ___ ___ Have you ever had metal fragments removed from your eyes? ___ ___ Have you ever been struck by a gun shot, B.B. or shrapnel? All of the above should be obvious. If they answer “yes” to any of these, it needs to be pursued thoroughly. Any potential subject that reports even the possibility of having metal in their eyes needs to be check with an eye orbit x-ray. Despite common misconception, there are many people who have bits of metal in their eyes and have do idea about it. ___ ___ Do you have any physical disabilities? Type? ________________________________________________________________________________ We would need to know this in case they needed help getting to/from on/off the scanner. ___ ___ ___ ___ Do you have any involuntary motor disorders? Type? ________________________________________________________________________________ If this would lead to movement during the scan, they should be rejected. Have you ever experienced claustrophobia? When? _______________________________________________________________________________ This should be self-explanatory. ___ ___ Do you have any back problems that would prevent you from lying still for up to 2 hours? This should be self-explanatory. Female Subjects ___ ___ Are you or is there a chance you are pregnant? Pregnant women should be rejected. It may be appropriate in certain protocols to include a formal pregnancy testt. ___ ___ Do you have an intrauterine device (IUD)? This needs to be followed up. We would need to confirm with their doctor that the device contained no metal (usually copper). Finally, there could be problems with severely obese persons fitting into the scanner. We should pay attention to the weight-height ratio. There are actually safety parameters build into the scanner which prevent its operation if the weight-height ratio is out of limit. MR Screening, Key, Rev 03/07/01, WI, Page 3