ahmed.attia_Short-segment Transpedicular Screw Fixation of
advertisement

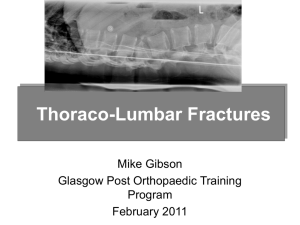
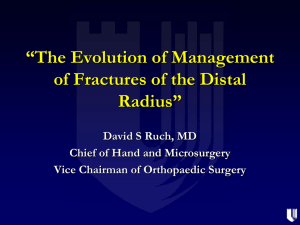
Short-Segment Transpedicular Screw Fixation of Unstable Traumatic Thoracolumbar Spine Fractures Ahmed M. Seleem, MD , Alaa A. Farag MD and Moataz A. Elawady MD Banha Faculty of Medicine ABSTRACT: Background: Thoracolumbar spine fractures are common in the young healthy population. The most common causes of these fractures are high-energy traumas, traffic accidents or falls from heights. Fractures can be followed by neurological deficit, which is a direct consequence of the spinal cord and/or root(s) damage. Fractures are treated with surgical or nonsurgical methods. Transpedicular screw fixation is one of the methods of surgical treatment objective: The aim of the paper was to evaluate the results of the posterior short-segment transpedicular screw fixation in the treatment of unstable traumatic fractures of the thoracolumbar spine. Patient and methods: This retrospective study included fifty patients with the diagnosis of thoracolumbar traumatic spinal fracture without posttraumatic neurologic deficit in the neurosurgical department of Banha University Hospital. They were operated upon with posterior instrumentation between January 2006 and January 2012. Results: Fifty (28 males and 22 females) with age ranging between 16 and 66 years (mean 41.8, St.D. 11.3) were operated upon by posterior transpedicular screw fixation. According to the ASIA scoring system all patients were grade E. The mean kyphotic deformities measured preoperatively was 19.2 degrees (±5.5 degrees) and at within 12 months follow-up, was 8.0 degrees (±3.6 degrees). The mean mid-sagittal diameter improved from 9.2 mm (±3.1 mm) before surgery to 15.1 mm (±0.8 mm) at the 12 months follow-up visit. Conclusion: By applying the transpedicular screw fixation of the unstable fractures of the thoracolumbar spine, a stable fracture fixation can be achieved. This kind of fixation prevents secondary spine deformities. INTRODUCTION: The thoracolumbar region is generally accepted as that part of the spine formed by vertebrae from the 11th thoracic to the 2nd lumbar(7). Spine fractures, especially fractures accompanied with the spinal cord injury, pose a difficult surgical, social and economic problem(6). The three major trauma mechanisms for thoracolumbar spine fractures are rotation/translation, distraction, and compression(1,15). Most thoracolumbar burst fractures are stable injuries that can be treated nonsurgically(2). Regardless of neurologic deficits, unstable burst fracture that have retropulsed bone fragments compromising the canal requires surgical interventions such as decompression of neural structures, correction of spinal deformities and stabilization.(13,15) The success of the treatment depends on the initial medical treatment, radiological diagnosis, anatomical reduction, surgical decompression of the spinal canal (if needed) and surgical stabilization (8). In cases of neurological damage, it is necessary to determine the exact grade of mobility impairment and of sensory functions(5). The classification and gradation of neurological damage in patients with the fractures of thoracolumbar spine are determined according to the ASIA (American Spinal Injury Association) score(1,14). This paper presents our experiences in the surgical treatment of thoraco-lumbar fractures by transpedicular screw fixation in patients who did not have any neurological damage. PATIENTS AND METHODS: Study design: This is a retrospective study of the data of fifty patients who were hospitalized with the diagnosis of traumatic thoracolumbar spinal fracture without posttraumatic neurologic deficit in the neurosurgical department of Banha University Hospital. There were operated upon with posterior short-segment instrumentation between January 2006 and January 2012. Preoperative assessment: Patients were clinically evaluated for type of injury, extent of Neurological deficit (ASIA grade) (Table 1)(5). Anterior- Posterior (AP) and lateral Plain Radiographs, Magnetic Resonance Imaging (MRI) and 3D-Computerized Tomography (3D-CT) scan was carried out in all patients. The segmental kyphosis angle was measured on lateral radiographs as the angle between the superior endplate of the first uninvolved vertebra proximal to the affected segment and the first uninvolved vertebra distal to the affected segment. Based on computerized tomography and magnetic resonance images of the patients, we evaluated intracanal fragments, the presence of pedicle and laminar fractures, posterior ligamentous complex status and the presence of medullary edema. Table 1: Asia Impairment Scale A = Complete: No motor or sensory function is preserved in the sacral segments S4-5. B = Incomplete: Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5. C = Incomplete: Motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3. D = Incomplete: Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more. E = Normal: motor and sensory function are normal Operative technique: Our surgical procedure was attempted to reach the retropulsed bone fragments through performing both laminectomy and minimal facetectomy. In prone position, we made a midline skin incision to expose the laminae 1 or 2 levels above and below the injured levels. We performed blunt dissection until the facet joints on both sides were seen. After routine laminectomy, we removed facet joints minimally to expose nerve root of both sides. Then, beneath the dural sac, we could push the retropulsed bone fragments down into the fractured vertebral body to their rightful position in the burst vertebral body. The manipulation was ought to be performed with great care to avoid damage to the neural structures. This was a crucial procedure to decompress the neural canal without removal of the retropulsed bone fragments. After the posterior decompression and bone fragment repositioning, the transverse processes, laminae of above and below level, and other posterior bony surfaces were decorticated for posterolateral fusion. Then, we carried out the classical short-segment pedicle screw instrumentation (transpedicular screw and rod instruments). Finally, we embedded sufficient amount of harvested bone fragments and artificial bone chips in the posterolateral sides of the column (posterolateral fusion) Follow up: The outcome was evaluated with (ASIA)(5) scale after three months, six months and one year following surgery. Plain x-Ray both anteroposterior and lateral views and 3D Computed Tomography were done postoperatively. The segmental kyphosis angle and the extent of collapse were measured on lateral radiographs at each visit. The presence of fusion was determined from two plain radiographs and was verified with CT scan. RESULTS Patient criteria: Fifty (28 males and 22 females) with age ranging between 16 and 66 years (mean 41.8, St.D. 11.3) were operated upon by posterior transpedicular screw fixation. According to the ASIA scoring system all patients were grade E. The distribution of fractures was as shown in Figure 1. The causes of these fractures were fall (23 patients), motor vehicle accidents (20 patients) and direct blunt trauma (7 patients). 16 14 12 10 8 6 4 2 0 D11 D12 L1 L2 Fig. 1: Distribution of levels of fractures Surgical outcome: Postoperative hospitalization: The average postoperative hospitalization was 9 days (range 5 – 14 days). Follow up: The average follow up period was 8.9 months (range 3 – 12 months). Radiological outcome: Preoperatively, most patients experienced loss of more than 40% of the vertebra body’s height and compromise of more than 25% in canal. Its overall mean values was 42.5% (±11.5%) and 28.6% (±10.2%), respectively. No statistically significant correlation appeared between the canal compromise and loss of vertebral body height (p>0.05). However, the mean kyphotic deformities, measured preoperatively and at within 12 months followup, were 19.2 degrees (±5.5 degrees) and 8.0 degrees (±3.6 degrees). The mean mid-sagittal diameter improved from 9.2 mm (±3.1 mm) before surgery to 15.1 mm (±0.8 mm) at the 12 months follow-up, with a significant difference between preoperative and postoperative values (p<0.01). Complications: Intraoperatively, dural tear occurred in two patients without no postoperative cerebrospinal fluid (CSF) leak. Superficial wound infection occurred in 3 patients and responded to antibiotic treatment (3rd generation Cephalosporins). No patient experienced neurological worsening. Screw fracture was observed in two patients on the 3-month follow up visit and required pedicle substraction osteotomy operation later on. a b c Fig. (2): a and b preoperative CT scan with 3D reconstruction of L1 fracture, c is postoperative x ray of the same patient a b c Fig. (3): a and b preoperative CT scan with 3D reconstruction of L1 fracture, c is postoperative x ray of the same patient DISCUSSION: In general, the treatment of thoracolumbar vertebral fractures is highly controversial. The vertebral stability after fracture constitutes an important part of the conflict(4). From the literature review, it can be established that various treatment methods ranging from conservative treatment to early surgical treatment have been used. The most important factor determining the treatment strategy is whether the patient has a neurological injury, and if yes, whether it is progressive or not. Since the concepts and definitions have not yet been agreed upon, different treatment approaches have evolved and continue to evolve(3,25,27). The aim of the treatment of spinal fractures is to achieve a painless, balanced and stable spine, healthy neurological function, the highest degree of spinal motion and to enable the patient to move in a short period of time(7,18). Surgical treatment is superior to conservative treatment in certain respects. Surgery provides spinal alignment and allows a better reduction of the fracture fragments. Canal width is more efficiently preserved regarding preventing a damage to neurological functions. It also prevents complications developing secondary to plaster cast or long-term bed rest. Due to its ability to provide a high degree of stability, patients can be mobilized earlier. Hence, rehabilitation can be initiated earlier(14,19,22). Posterior surgery is performed primarily in the treatment of burst fractures without neurological deficit. With the effects of lordosis and posterior distraction force applied during posterior decompression, intracanal tissues are expected to be displaced anteriorly(12,13,18,20,27). Dunn, 2009 concluded that short segment posterior instrumentation is a safe and effective option in the treatment of unstable thoracolumbar fractures as a standalone measure(11). McLain et al. detected early failure of this technique(18). In a retrospective study of 28 patients, Sanderson et al. (1999) performed short segment posterior instrumentation without fusion in one level above and below the fractured vertebra and followed up the patients for two years. Implant failure was screw breakage in four patients (prevelation is 14%)(24). In a prospective randomized study, Alanay et al. (2001) evaluated the efficacy of transpedicular grafting and established that similar results were obtained with and without grafting(2). In a prospective clinical study, Wang et al. compared the results of surgical treatment with and without fusion in thoracolumbar burst fractures. In that study, a total of 58 patients who were neurologically intact, with a kyphosis angle greater than 20° and a canal narrowing and collapse in vertebral height of greater than 50% were enrolled. As a result of that study, no marked difference was observed in kyposis angles between the two groups. Radiographic parameters were found to be statistically better in the non-fusion group. Implant failure was screw breakage in eight patients (prevelance 13.7%), five of whom were in the fusion group whereas 3 were in the nonfusion group. The authors suggested that the short term outcomes of short segment pedicular fixation without fusion in the treatment of thoracolumbar fractures were satisfactory. Additionally, they suggested that the advantages of nonfusion surgery included the absence of donor site related problems, preservation of motion segments, decreased blood loss, and the shortened duration of the surgery(26). Li-yang et al. published the results of a 5 years prospective randomized clinical study of 73 patients who underwent posterior short segment fixation with and without fusion for thoracolumbar burst fractures. Among radiological results, local kyphosis angle and loss of kyphosis angle correction were taken as the basis. As a result, no radiological or clinical differences were detected between the two groups. The duration of the operation and blood loss were found to be statistically significantly lower in the non-fusion group (p<0.05)(17). In a prospective study by Robertson and Wray, graft donor sites were examined in 106 patients who underwent posterior spinal fusion 3.6, and 12 months after the surgery and it was demonstrated that the pain increased in the first 6 months and tended to decrease afterwards(23). Also, in the study by Dai LY et al. pain was observed but not considered to be a major problem. However, they emphasized that the presence of these findings are irrefutable. Consequently, they reported that posterolateral bone grafting was not necessary when posterior short segment fixation was performed in selected patients (Dennis type B patients with a load sharing score of <6)(10,17,21). Posterolateral bone grafting was done in all of our patients. CONCLUSION By applying the transpedicular screw fixation of the unstable fractures of the thoracolumbar spine, a stable fracture fixation can be achieved. So early ambulation, rapid return to work and less rehabilitation costs could be achieved. This kind of fixation prevents secondary spine deformities. REFERENCES 1. Aebi M. Classification of thoracolumbar fractures and dislocations. Eur Spine J 2009;19 (suppl.1): 2-7. 2. Alanay A, Acarolu E, Yazici M, Oznur A and Surat A: Shortsegment pedicle instrumentation of thoracolumbar burst fractures: does transpedicular intracorporeal grafting prevent early failure. Spine 2001, 26(2):213-217. 3. Alici E, Berk H, Akseki D and Baktiro_lu L: Burst fractures of the thoracolumbar spine. Turkish J. Spine Surg 1992, 3: 8-20. 4. Altay M, Ozkurt B, Aktekin CN, Ozturk AM, Dogan O and Tabak AY: Treatment of unstable thoracolumbar junction burst fractures with short- or long- segment posterior fixation in magrel type a fractures. Eur Spine J 2007, 16:1145-1155. 5. 6. American Spinal Cord Injury Association: Standards for neurological and functional classification of spinal cord injury, revised. Chicago, IL: American Spinal Cord Injury Association 1992. Anderson PA, Rivara FP, Maier RV and Drake C: The epidemiology of seatbelt-associated injuries, J Trauma 1991, 31, 60– 67. 7. Berk H: Sirt-Bel Omur Kiriklari: TOTB_D J 2008, 7(1-2): 20-34. 8. Boerger TO, Limb D and Dickson RA: Does canal clearance affect neurological outcome after thoracolumbar burst fracture? J Bone Joint Surg [Br] 2000, 82-B:629-35. 9. Butt MF, Farooq M, Mir B, Dhar AS, Hussain A and Mumtaz M: Management of unstable thoracolumbar spinal injuries by short segment spinal fixation. International Orthop 2007, 31:259-264. 10. Cho DY, Lee WY and Sheu PC: Treatment of thoracolumbar burst fractures with polymethyl methacrylate vertebroplasty and shortsegment pedicle screw fixation. Neurosurgery 2003, 53(6):13541360. 11. Choi DY, Kim YB, Yeo SJ, Park SW and Hwang SN: One stage spondylodesis for the bursting fracture of the thoracolumbar spine though unilateral posterior approach. J Korean Neurosung Soc 2004, 35:379-382. 12. Dunn RN: Short-segment posterior instrumentation of thoracolumbar fractures as standalone treatment. SA Orthopaedic Journal Winter 2009. 68-7. 13. Floman Y: Posterior instrumentation in the management of thoracolumbar injuries. Argenson C(eds) Thoracolumbar spine. New York Raven Press 1993, 279-306. 14. Jacobs RR, Nordwall A and Nachemson A: Reduction, stability, and strength provided by internal fixation systems for thoracolumbar spinal injuries. Clin Orthop, 1982; 171:300-8. 15. Knop C, Bastian L, Lange U, Oeser M, Zdichavsky M and Blauth M: Complications in surgical treatment of thoracolumbar injuries. Eur Spine J, 2002, 11(3):214-226. 16. Li KC, Hsieh CH, Lee CY and Chen TH: Transpedicle body augmenter: a further step in treating burst fractures. Clin Orthop Relat Res, 2005, 436:119-125. 17. Li Yang Dai, Sheng Dan Jiang, MSci, Xiang Yang Wang and Lei Sheng Jiang: A review of the management of thoracolumbar burst fractures. Surgical Neurology, 2007, 67: 221-231. 18. McLain RF, Sparling E and Benson DR. Early failure of shortsegment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg (Am) , 1993;75:162-7. 19. Milenković S, Saveski J, Trajkovska N, Vidić G and Radenković M: Transpedicular Screw Fixation of Thoracolumbar Spine Fractures. Scientific Journal of the Faculty of Medicine in Niš, 2010; 27(2): 63-68. 20. Modi HN, Chung KJ, Seo IW, Yoon HS, Hwang JH, Kim HK, Noh KC and Yoo JH: Two levels above and one level below pedicle screw fixation for the treatment of unstable thoracolumbar fracture with partial or intact neurology. Journal of Orthopaedic Surgery and Research, 2009, 4:28. 21. Ahmed NMS: Vertebroplasty in combination with pedicle screw instrumentation: A new trend in traumatic thoracolumbar fractures. Pan Arab Journal of Neurosurgery April 2010. 14(1) 22. Parker JW, Lane JR, Karaikovic EE and Gaines RW: Successful shortsegment instrumentation and fusion for thoracolumbar spine fractures: a consecutive 4 1/2-year series. Spine, 2000, 25(9):11571170. 23. Robertson PA and Wray AC: Natural history of posterior iliac crest bone graft donation for spinal surgery: a prospective analysis of morbidity. Spine, 2001, 26: 1473-1476. 24. Sanderson PL, Fraser RD, Hall DJ, Cain CMJ, Osti OL and Potter GR: Short-segment fixation of thoracolumbar burst fractures without fusion. Eur Spine J , 1999, 8 : 495-500. 25. Tezeren G and Kuru I: Posterior fixation of thoracolumbar burst fracture. Short-segment pedicle fixation versus long-segment instrumentation. J Spinal Disord Tech, 2005, 18:485-488. 26. Wang XY, Dai LY, Xu HZ and Chi YL: The loadsharing classification of thoracolumbar fractures: an in vitro biomechanical validation, Spine, 2007, 32, 1214–1219. 27. Yue JJ, Sossan A, Selgrath C, Deutsch LS, Wilkens K, Testaiuti M and Gabriel JP: The treatment of unstable thoracic spine fractures with transpedicular screw instrumentation: a 3-year consecutive series. Spine, 2002, 27(24):2782-2787. الملخص العربي التدخل الجراحي الخلفي باستخدام مسامير لكسور المنطقة الفقارية الصدرية-القطنية غير المتزنة: تقييم المردود السريري و التصويري بيانات أساسيي :إن دواعي اتديد ا اتا اح ي ات لفي تكسيوح اتمنطقي اتفقرحةي اتريدحة - اتقطني دشما اتكسوح غيح اتمدزن غيح اتمر وب بأي لا عرب . الغييي أاحة ييذ ييرا اتد احسي ي تدقي يييس اتم ييحدود اتسي يحةحي و اتدر ييوةحي تلد ييد ا اتا اح ي ي ات لف تكسوح اتمنطق اتفقرحة اتردحة -اتقطني غيح اتمدزن . تصميم الد اس :دحاس بأثح حاع ت رالذ سحةحةه ومحااع األب رث. الط ق ف اتفديح مير بيين ينيريح 2006وةنيريح 2012دبيين أن 50محةضير ديد اايحي ت يس دييد ر ا اح ييير لفييير بسييب كسييح غيييح مدييزن برتمنطق ي اتفقرحة ي اترييدحة -اتقطني ي ودييد دييس ددب ي اتمحض ي س يحةحةر و درييوةحةر برسييد داس األشييع اتسيييني واتدرييوةح اتطبق ي مدعييدد اتمقييرط ثرث ي األبعرد. النتائج ااحي اتدد ا اتا اح األمرم بسب كسح برتمنطقي اتفقرحةي اتريدحة -اتقطنيي ف ي ي 50محةضي يير ( 28مي يين ات ي يركوح و 22مي يين اإني ييرثب وأثبدي ييذ اتدقي ييرحةح اتطبي ي ي د سي يين ات رت ي ي اتدروةحة واتثبرذ اتفقرحي اتميكرنيك بكا ات رالذ. الخالص ::أثبدذ اتدحاس فعرتي و أمرن اتدد ا اتا اح اتمنطق اتفقرحة اتردحة -اتقطني غيح اتمدزن . تلدد ا اتا اح ي ات لفي تكسيوح