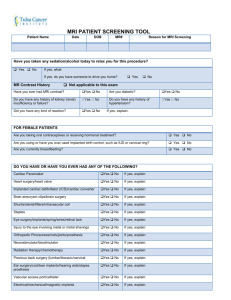
MRI screening form (Office document, 1488kB)
advertisement
")
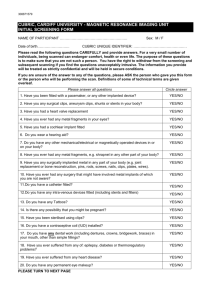
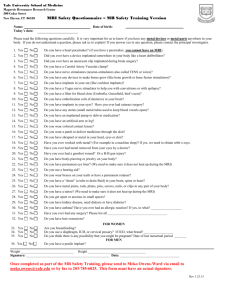
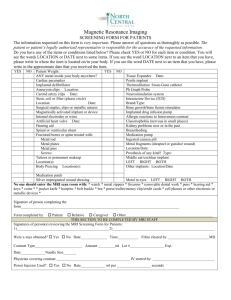
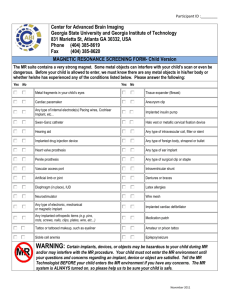
MAGNETIC RESONANCE IMAGING INITIAL SCREENING FORM NAME OF PARTICIPANT.............................................................................. Date of birth……………………… Sex: M / F Weight in kg……… or Stones/lbs Height in cm or m……………… Please read the questions on this screening form CAREFULLY. Your safety in the magnetic environment is our primary concern. THIS IS VERY IMPORTANT. For a very small number of individuals, being scanned can be uncomfortable, or endanger health or even life. The purpose of these questions is to make sure that you are not such a person. The information you provide will be treated as strictly confidential and will be held in secure conditions. If you are unsure of the answer to any of the questions, please ASK the person who gave you this form or the person who will be performing the scan. Definitions of some of the more technical terms are given overleaf. I wish to be screened by the same gender YES/NO* Please answer all questions Bold answer 1. Have you been fitted with a pacemaker, artificial heart valve, cochlear implant or any other implanted device? YES/NO 2. Have you any surgical clips, aneurysm clips, shunts or stents in your body? YES/NO 3. Have you ever had any metal fragments in your eyes? YES/NO 4. Have you been exposed in your life to metal debris as a result of welding, grinding, filing, sawing or drilling of metal either occupationally or recreationally? YES/NO 5. Do you wear a hearing aid? YES/NO 6. Have you ever had any metal fragments, e.g. shrapnel in any other part of your body? YES/NO 7. Have you any surgically implanted metal in any part of your body (e.g. joint replacement or bone reconstruction)? YES/NO 8. Have you ever had any surgery that might have involved metal implants of which you are not aware? YES/NO 9. Is there any possibility that you might be pregnant? YES/NO 10. Do you have a contraceptive coil (IUD) installed? YES/NO 11. Have you been sterilised using clips? YES/NO 12. Do you have any dental work (including dentures, crowns, bridgework, braces) in your mouth, other than simple fillings? YES/NO 13. Have you ever suffered from any of: epilepsy, diabetes or thermoregulatory problems? YES/NO 14. Have you ever suffered from any heart disease? YES/NO 15. Do you have any tattoos? Do you have any permanent eye makeup? YES/NO 16. Are you wearing any skin patches? (eg. Nicotine ) YES/NO I have read and understood the questions above and have answered them correctly. SIGNED………………………………....................................... DATE………………………… In the presence of ………………………………….. (Name) ………………………………….. (Signature) Page 1 of 2 STON UNIVERSITY - MAGNETIC Appendix RESONANCE IMAGING UN Definition of Technical Terms PACEMAKER: An electronic device that is surgically placed in the patient's body and connected to the heart to control the heartbeat. The safe operation of a pacemaker can be temporarily or permanently disrupted if a person with a pacemaker goes near an MRI scanner. COCHLEAR IMPLANT: An electronic medical device that bypasses damaged structures in the inner ear and directly stimulates the auditory nerve, allowing some deaf individuals to learn to hear and interpret sounds and speech. ANEURYSM CLIP: A surgically implanted metal clip used to cut off blood flow through the neck of an aneurysm. An aneurysm is a deformity of a blood vessel in the body, which can swell and burst causing a haemorrhage. SHUNT: A surgically implanted connector, which allows passage of fluid between two parts of the body. A common use of a shunt is to allow fluid to drain away from the brain, thus reducing pressure in the brain. May also describe a tube which allows blood to be moved from one part of the body to another. STENT: A surgical implanted device that is inserted into a blood vessel to provide support, keep the vessel open and improve blood flow. Sometimes used in other fluid carrying vessels in the body such as bile ducts etc. THERMOREGULATORY PROBLEMS: Thermoregulation is the body’s in-built ability to keep all parts of your body at their correct temperature. Some illnesses prevent the person from properly controlling the temperature of their body. If you think you may have such an illness, please answer “YES” and discuss it with the person who gave you the form, or the person who is in charge of the scan. Page 2 of 2