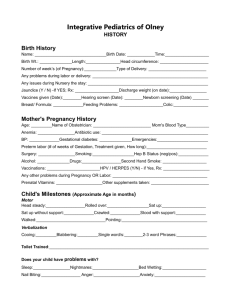
birth history
advertisement

THE CENTER FOR PEDIATRIC & ADOLESCENT MEDICINE Revised 01/17/05 FAMILY HISTORY Patient’s Name___________________________________________ Date _______________ FAMILY MEMBER AGE LIST ANY HEALTH PROBLEMS Mother ____ ___________________________________ Father ____ ___________________________________ Sibling ____ ___________________________________ Sibling ____ ___________________________________ Sibling ____ ___________________________________ Sibling ____ ___________________________________ Sibling ____ ___________________________________ Sibling ____ ___________________________________ List any family member related to the patient who has any of the following diseases Miscarriages______________ Allergies, Hay fever, Asthma________ Liver Disease_________ Mental Retardation_________ High Cholesterol__________________ Intestinal Disease______ Birth defects______________ Bleeding Disorders________________ Any Other Diseases_____ Seizures__________________ Rheumatic Heart Disease___________ _____________________ Diabetes__________________ Kidney Disease___________________ EXPOSURE Does anyone in your household smoke, drink alcohol, chew smokeless chewing tobacco, or drugs? Y / N If yes who? ______________________________________ Does anyone in the household have a gun? Yes / No If yes who?_________________________ BIRTH HISTORY Pregnancy: Delivery: Full term or Premature ____ Weeks Gestation Vaginal or C-section Neonatal Course Any Complications in the nursery? ______________________________ DIETARY HISTORY Present Eating Habits: Infant : Formula Type _________ Solid Foods _______________ Child : Good or Picky Eater Do you have well water ? Y or N DEVELOPMENTAL HISTORY List age when accomplished each of the following: INFANT Sat up alone ______ Said 1st Words ______ ______ Said 1st Sentence ______ 1st Teeth ______ Walked Toilet Trained ______ SCHOOL AGE Present Grade ______ Any Problems _____________________________________________ HOSPITALIZATIONS List all Hospitalizations, age and diagnosis, not including surgeries Diagnosis Age Diagnosis Age _________ ______ ________ ______ _________ ______ ________ ______ SURGERIES List all surgeries, age and diagnosis Diagnosis Age Diagnosis Age _________ ______ _________ ______ _________ ______ _________ ______ MAJOR ILLNESSES List any past major illnesses (i.e. Urinary tract infections, pneumonias, strep throat etc…….) Diagnosis Diagnosis ________________________________ _________________________________ ________________________________ _________________________________ INJURIES List all injuries (i.e. Broken bones, skull fractures, or major injuries) Diagnosis ________________________________ Diagnosis _________________________________ ________________________________ _________________________________ MEDICATIONS Please list all current medications your child is taking __________________________________________________________________________________ __________________________________________________________________________________ ALLERGIES TO ANY MEDICATIONS List all medications to which your child is allergic to __________________________________________________________________________________ __________________________________________________________________________________ UPDATED ( Every 2 Years) 1)__________ 2)__________ 3)__________ 4)__________ 5)__________ 6)__________ 7)__________ 8)__________ 9)__________ 10)_________ PATIENT’S NAME____________________________________________ DOB_________________ Revised 01/17/2005 IMMUNIZATIONS This section to be completed by the nurse or physician DTAP/TD Pediarix 1) ________ 1) ________ 1) ________ 1) ________ 1) ________ 1) ________ 2) ________ 2) ________ 2) ________ 2) ________ 2) ________ 2) ________ 3) ________ 3) ________ 3) ________ 3) ________ 3) ________ 4) ________ 4) ________ 4) ________ 5) ________ 5) ________ Varivax Prevnar 7 IPV Hib 1)________ 1)________ 1)________ 1)________ 2)________ 2)________ 2)________ 2)________ 2)________ 4) ________ MMR 4) ________ Pnu-23 Immune 1)________ 3) ________ HEP A HBV Td Booster Menomune 1)________