RETINOPATHY OF PREMATURITY - Great Neck Public Schools
advertisement

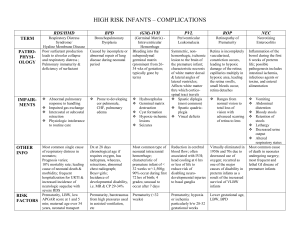
Retinopathy of Prematurity 1 Running Head : RETINOPATHY OF PREMATURITY Retinopathy of Prematurity. (Your name goes here) Great Neck South High School Retinopathy of Prematurity 2 Retinopathy of Prematurity Newborn infants with respiratory trouble may need to go straight into an infant incubator, which keeps the baby’s core temperature at 37C, humidifies the air, and adds extra oxygen to compensate for weak breathing (Retinopathy of Prematurity, 2005). However, this health care option has a very serious risk associated with it, blindness. Retinopathy of Prematurity (ROP) is a disorder of the blood vessels of the retina, which is a light sensitive multilayer of tissues at the back of the inner eye. It acts like a film in a camera, and converts these images into electrical signals, sending them via the optic nerve to the brain. Retinopathy of prematurity is caused by abnormal growth of the retina vessels in the eye (American Association, 2005). The more premature the baby and the lower the birth weight, the greater the risk for developing Retinopathy of Prematurity (Retinopathy of Prematurity, 2005). Many premature babies develop blindness as a result of retina damage caused by high oxygen levels in their blood. Premature babies have the highest risk (International Committee, 2000). All infants have immature vessels in the eyes in the condition of being in the high oxygen (Baby harming, 2005). This is because babies who are born prematurely still have a growing retina, which usually doesn’t finish growing in full term babies until a few weeks to months after birth. High oxygen levels result in the growth of abnormal blood vessels, or can damage and scar existing blood vessels in the retina. In the most serious cases, detachment of the retina from the back of the eyes can occur, resulting in blindness (Retinopathy of Prematurity, 2005). Also, the abnormal vessels growth produces fibrous scar tissue and those vessels come together to shape the eye. The abnormal vessels of retina can be pulled, detached, which in some cases will result in blindness if there is enough scar tissue formed (Baby harming, 2005). There are three different zones for the retina that affected by Retinopathy of Prematurity. When babies are affected on the Zone 1 then it is worse then Zone 2. Zone 1 Retinopathy of Prematurity 3 includes the area of macula which is the part of retina that serves central vision. And also, Zone 1 is centered round the optic nerve of the eye at the back. Zone 2 has a shape of doughnut that surrounds Zone 1. The outer edge goes out to outer, most anterior edge of the nasal retina. In addition Zone 3 has crescent shape of retina. It is a anterior to Zone 2 and also is temporal part of the eye (American Association, 2005). The Zone 1’s disease is sometimes invariable to treat it. However, for Zone 2 and Zone 3, from 12.5% to 76.9% it can be treated with treatment or treated without treatment. It might bring the sites back to the babies, but the cases of being complete sight are rare. (Sharma et al., 2007) Retinopathy of Prematurity progresses through five stages ranging from mild to severe, which depends on the location and degree of retinal scarring that, has occurred. The first stage is classified by mild abnormal blood vessel growth. If removed from high oxygen levels, the patient likely will recover with normal vision without having had any treatment. The second stage is identified by the presence of blood vessels with moderately abnormal growth, while the third shows signs of blood vessels with severely abnormal growth. In this stage, the blood vessels grow into the center of the eye instead of following their normal path along the retina. The fourth stage is classified as abnormal blood vessels with a partially detached retina, but the macula (center of the retina) is attached. The surgeries bring the vision back by reattaching or making new normal vessels to grow in the retina. In the fifth and final stage, the retina is completely detached, surgery is no longer possible, and the infant is blind (Oxygen Restrictions, 2000). There are two major treatments for Retinopathy of Prematurity. The first involves the use of cryotherapy (freezing) the retinal tissue, a procedure that has been used since the 1970’s (Laura & Richard, 2006). Today, cryotherapy is combined with diode laser photocoagulation. In this procedure, a freeze probe is held onto the outside of the eye and a laser is used to destroy a small part of the damaged retina or the abnormal vessel. Removing Retinopathy of Prematurity 4 of damaged or abnormal vessel allows the new normal vessels to grow again in the eye. This brings the eye sight back in most of the case (Laura & Richard, 2006). Another way is called, vitrectomy. This procedure removes the vitreous gel in the retina which allows the retina to pull away from the wall of the eye. Then it settles back against the wall of eye and reattach to it in normal way. In addition, a scleral buckling can be helpful, too. A band of silicone plastic is located around the outside wall of eye. The band pushed or support the wall of eye to the detached retina vessels so that it can be reattaches again to the wall of the eye (American Association, 2005). Despite major advances in the treatment of ROP, this disease remains a significant cause of blindness in the developed world (Donahue, 2002). Since oxygen appears to be causing the damage, researchers continue to try and find ways to reduce oxygen levels in the blood of susceptible infants, while providing optimal oxygenation to the lungs and other organs (Morzejewska, 2006). Also, Vitamin E supplementation has been shown to help or prevent the gap between the vessels or detachment of the vessels. It supports the involvement of oxygen radical induced autoxidation in the gap or detachment place to reattach the blood vessels again (Rao & Wu, 1996). Preventing premature births would be a simple solution to preventing ROP. However, this is an unlikely solution since early birth is sometimes inevitable. Word Count: 980 Retinopathy of Prematurity 5 References American Association for Pediatric Opthalmology and Strabismus. (2005). Retinopathy of Prematurity areas. Retrieved January 20, 2008, from http://www.aapos.org/displaycommon.cfm?an=1&subarticlenbr=227 Baby harming medical research frauds about retinopathy of permaturiy. (2005). Retrieved October 7, 2007, from http://www.retinopathyofprematurity.org/index.htm. Donahue, S. P. (2002). Retinopathy of prematurity. British Journal of Ophthalmology, 86, 1071. International Committee for the Classification of Retinopathy of Prematurity. (2005). Arch Ophthalmol. 123(7), 991-999. Laura K & Richard L. (2006). Understanding Retinopathy of Prematurity. Vision Enhancement Journal.-missing information Modrzejewska, M. (2006). Retinopathy of prematurity: clinical findings and current opinions on diagnosis and treatment. Ann Acad Med Stetin, 52(1), 73-8. Oxygen Restrictions Can Be Eased for Premature Infants with Blinding Eye Disease (2000). Retrieved October 2, 2007, from http://www.nei.nih.gov/news/pressreleasees/ 020700.asp. Rao, N. A., & Wu, G. S. (1996). Oxygen free radicals and retinopathy of prematurity. The British Journal of Opthalmol, 80(5), 387. Retinopathy of prematurity. (1995). Retrieved October 7, 2007, from http://www.rnib.org.uk/ xpedio/groups/public/documents/publicwebsite/public_rnib003663.hcsp. Retinopathy of prematurity. (1998). Retrieved December 15, 2007, from http://www. schepens .com/ retinopathy_of_prematurity.htm. Retinopathy of Prematurity. (2005). Retrieved October 27, 2007, from http://www.childrens Retinopathy of Prematurity 6 hospital.org/az/Site1524/mainpageS1524P0.html.