Laparoscopy
advertisement

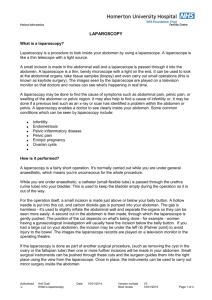
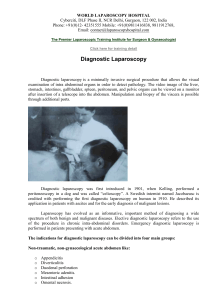
Laparoscopy for abdominal/pelvic pain This information is intended for those with lower abdominal/pelvic pain who may be considering or undergoing a laparoscopy. It aims to summarize the role of laparoscopy for diagnosing and treating lower abdominal/pelvic pain. Laparoscopy (key-hole surgery) can be performed for diagnosis (diagnostic laparoscopy) or treatment (therapeutic laparoscopy). This information aims to explain the difference between the two procedures, along with the risks and complications in order to assist in decision making. What is laparoscopy ? Laparoscopy is a type of surgical procedure that allows a surgeon to access the inside of the abdomen (tummy) and pelvis by making small incisions in the skin. It is also known as keyhole or minimally invasive surgery. The laparoscope is the instrument which is used for the procedure. It is a thin telescope with a light source and a video camera which allows inspection of the abdomen/pelvis and sends pictures of the inside of the abdomen or pelvis in real time to a TV screen/monitor. How is a laparoscopy carried out ? Laparoscopy is carried out under general anaesthetic, so you will be asleep during the procedure. A small 1-2 cm cut is made, usually near the belly button, through which the laparoscope is inserted. A tube is also connected to a carbon dioxide gas pump. This is used to inflate your abdomen so that the surgeon can easily look around. The carbon dioxide gas dissipates after the operation. If surgical treatment is being carried out during the laparoscopy, a further two or three small 5 mm cuts are made on the abdomen. Small surgical tools are then inserted which the surgeon uses to cut, move and grab the tissues. After the procedure, the gas is let out of your abdomen, the cuts are closed using stitches and dressings are applied. It is important that you avoid the risk of pregnancy, either by avoiding intercourse, or by using barrier contraception before the laparoscopy. Laparoscopy is used for diagnosis (diagnostic laparoscopy) or for treatment (therapeutic laparoscopy) Diagnostic laparoscopy Laparoscopy is widely used to try to diagnose many different conditions including unexplained pelvic or abdominal pain. However, about 4 in 10 laparoscopies do not reveal any clear diagnosis (Howard 1993, Yasmin 2005). If your laparoscopy does not give a clear diagnosis, it is important that you ask your doctor for further advice. For example, many patients can benefit from being referred to a pain specialist. (Doyle 2005, Cox 2007) Therapeutic laparoscopy Therapeutic laparoscopy can be performed the traditional way or with robotic assistance (see below). Laparoscopic surgery can be used to treat several different conditions, including : - - - - Treating endometriosis.In women with endometriosis, cells from the womb lining (the endometrium) are found in other places inside the body. These include the lining of the wall of the pelvis, ovaries, Fallopian tubes, bladder and bowel. Removing or burning endometriosis tissue can help to relieve painful symptoms (Cochrane review, laparoscopic surgery for pelvic pain associated with endometriosis 2009). In severe cases, referral to a specialist centre may be required. Removing an inflamed or diseased appendix (Gaitan 2011) Removing a section of bowel which has been affected by conditions such as Crohn’s disease, diverticulitis, or endometriosis and which has not responded to medication. Repairing hernias, such as those in the groin Removing some or all of an organ that has been affected by cancer Removing fibroids.These are growths in the muscle of the womb. They are usually small and do not cause symptoms. Occasionally, if they do cause symptoms they can be removed. Dividing scar tissue inside the abdomen (adhesions) which sometimes affect some of the internal organs. Removing the womb (hysterectomy) see NICE IPG 239. However there is no good evidence that it will relieve symptoms of persistent pelvic pain, and indeed it may aggravate them Some of these procedures require specialist education and training. In our opinion patients should ask about the experience of the surgeon who will be doing the procedure and the outcomes, as well as the risk of adhesions. See information about safety below. See and Treat This is a form of therapeutic laparoscopy, assessing what the problem is and dealing with it at the same time. It is suggested by the Royal College of Obstetricians and Gynaecologists that for some conditions, such as endometriosis, “See and Treat” laparoscopy should replace diagnostic procedures. Thorough clinical assessment, examination and tests such as transvaginal ultrasound, MRI scan, CT scan before surgery are used to identify those who are suitable for “See and Treat” laparoscopy (Hebbar 2005, Ball 2008). Laparoscopy can be used to obtain a sample of tissue (biopsy), which is sent to a laboratory for testing. We encourage you to ask your clinician to biopsy areas of endometriosis, and areas that are suspicious, during diagnostic or therapeutic laparoscopy ( ESHRE Endometriosis Guideline 2013 ). A separate consent form may be needed for this as well as for therapeutic laparoscopy. You may want to ask the surgeon if it is possible to have a video (or photos ) of the surgery as a permanent record of the surgery. This may be useful to refer to in future. Robotic-assisted laparoscopy A recent development in laparoscopy is the use of robots to assist with procedures. This is known as robotic-assisted laparoscopy. During robotic-assisted laparoscopy, your surgeon will use a console located in the operating theatre to carry out the procedure by controlling robotic arms. The robotic arms hold a special laparoscopic camera and surgical equipment. Robotic-assisted laparoscopy allows surgeons to operate with increased precision and smaller cuts. It is now frequently used in urology and neurosurgery. Other areas such as gynaecology are in earlier stages of development. The advantages and disadvantages over traditional laparoscopy are still being debated. Recovery After laparoscopy, you may feel groggy as you recover from the effects of the anaesthetic. Some people feel sick or vomit. These are common side effects of the anaesthetic and should pass quickly. Before you leave hospital, you will be told how to keep your wounds clean and when to return for a follow-up appointment or to have your stitches removed, although dissolvable stitches are now often used. For a few days after the procedure, you are likely to feel some pain and discomfort where the incisions were made and you may also have a sore throat if a breathing tube was placed down your throat during the procedure. You will be given painkilling medication to help relieve the pain. Sometimes the gas used to inflate your abdomen can cause bloating and cramps. You may also have pain in the shoulder. This is because your diaphragm (the muscle between your chest and your abdomen that you use to breathe) can be irritated by the stretch from the gas, and this pain is radiated to the shoulder. These symptoms are nothing to worry about and should pass after a day or so once your body has absorbed any remaining gas. You may experience some vaginal bleeding. This should not be heavy and should only last a couple of days. You should use sanitary towels rather than tampons whilst this bleeding lasts, to avoid the risk of infection. Over the following days or weeks, it is likely you will feel more tired than usual, as your body is using a lot of energy to heal itself. Taking regular naps may help. The length of time to recover may vary from person to person depending on the treatment carried out. Safety and Complications Your hospital should tell you about your surgery and the different options that are suitable. They should tell you what you need to do in order to prepare for your laparoscopy. They should also inform you about the potential risks and side effects. Overall, a complication occurs in 5 out of every 1,000 laparoscopies. More complex procedures may carry higher risks ( Chapron 2001). Scar tissue inside the abdomen(adhesions) can occur after any surgery. Adhesions can be associated with infertility, persistent pelvic pain and small bowel obstruction (ten Broek 2013). You may want to discuss this risk with your surgeon and see whether you might benefit from having an anti-adhesion product introduced into your abdomen at the end of your laparoscopy to reduce the risk (Parker 2007, Kraemer 2011,Audebert, 2012, De Wilde 2012). Some procedures such as those for endometriosis pose an increased risk of adhesions. Minor complications such as post operative infection, bleeding and bruising around the site of the cut occur in 1-2 out of every 100 laparoscopies. Serious complications after laparoscopy are infrequent; however in such cases further laparoscopic or open surgery may be required. These complications include: damage to an organ, such as your bowel or bladder, which could result in the loss of organ function damage to a major artery damage to nerves air embolism: where gas bubbles collect in your veins and cause a blockage a serious allergic reaction to the general anaesthetic a blood clot developing in a vein, usually in one of the legs (deep vein thrombosis or DVT), which can break off and block the blood flow in one of the blood vessels in the lungs (pulmonary embolism) death : between 3 and 8 in 100,000 patients die as a result of complications. Other less serious complications can occur after discharge from hospital. If you are given a follow-up appointment, please make sure you attend. When to seek medical advice It is usually recommended that you have someone stay with you for the first 24 hours after your surgery. This is in case you experience any symptoms that suggest there could be a problem, such as: a high temperature of 38°C (100.4°F) or above chills increasing abdominal pain redness, pain, swelling and discharge around your wounds pain and swelling in one of your legs a burning or stinging sensation when urinating If you experience any of these symptoms during your recovery, you should contact the hospital where the procedure was carried out, your GP or NHS 111 for advice. If you don’t think that your laparoscopy has been successful, either in diagnosing or treating your condition, you should ask your surgeon or GP for further advice. Sometimes referral to another specialist is beneficial. References and further reading: De Wilde RL, Brölmann H, Koninckx PR, Lundorff P, Lower AM, Wattiez A, Mara M, Wallwiener M; The Anti-Adhesions in Gynecology Expert Panel (ANGEL). Prevention of adhesions in gynaecological surgery: the 2012 European field guideline.Gynecol Surg. 2012 Nov ESHRE Endometriosis Guideline September 2013 Hernando G Gaitán1,*, Ludovic Reveiz2, Cindy Farquhar3Editorial Group: Cochrane Menstrual Disorders and Subfertility Group Laparoscopy for the management of acute lower abdominal pain in women of childbearing age.2011 Jan. Jacobson TZ, Duffy JM, Barlow D, Koninckx P, Garry R5Editorial Group: Cochrane Menstrual Disorders and Subfertility Group Laparoscopic surgery for pelvic pain associated with endometriosis, 2009 Oct Kraemer B, Birch JC, Birch JV, Petri N, Ahmad U, Marikar D, Wallwiener M, Wallwiener C, Foran A, Rajab TK. Patients' awareness of postoperative adhesions: results from a multi-centre study and online survey Arch Gynecol Obstet. 2011 May;283(5):1069-73. RCOG Consent Advice 2: December 2008 SOGC Consensus Guideline for the Management of Chronic Pelvic Pain Part one 2005 ten Broek RP, Issa Y, van Santbrink EJ, Kruitwagen RF, Jeekel J, Bakkum EA, Rovers MM, van Goor H. Burden of adhesions in abdominal and pelvic surgery: systematic review and met-analysis.BMJ. 2013 Oct PPSN-WEB-011 Issue date: February 2014 Review date: February 2017