long term safety and efficacy of combination therapy with
advertisement

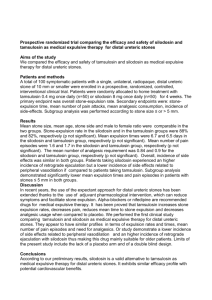
SAFETY AND EFFICACY OF VARDENAFIL 10 MG AND TAMSULOSIN 0,4 MG IN THE TREATMENT OF MEN WITH LUTS DUE TO BPH: A RANDOMISED, PLACEBOCONTROLLED STUDY M. Gacci, G. Vittori, G. Siena, M.A. Rossetti, N. Tosi, A. Lapini, S. Serni, M. Maggi, M. Carini INTRODUCTION Safety and efficacy of tamsulosin and vardenafil are well defined: however, there is no report regarding the safety and efficacy of combined therapy of both types of agents for LUTS/BPH men. The aim of our study was to compare the safety and efficacy of tamsulosin 0.4 mg/day vs. tamsulosin 0.4 mg/day plus vardenafil 10 mg/day in men with LUTS/BPH, in a randomized trial with 3 month follow up. MATERIALS AND METHODS Sixty men with persistent irritative urinary symptoms after 2 weeks run-in with tamsulosin 0.4 mg were randomized in 2 groups: group VAR (30 P.ts) undergone a combination therapy with tamsulosin 0,4 mg and vardenafil 10 mg (both one a day), while group PLA (30 P.ts) undergone a combination therapy with tamsulosin 0,4 mg and placebo (both one a day). IPSS (International Prostate Symptom Score), IPSS-B (International Prostate Symptom Score- Bother), IIEF-5 (International Index of Erectile Function, Version 5) and OAB-q (Over Active Bladder questionaire) scores, uroflowmetry data and post-voiding residual urine (PVR) were recorded at baseline (after run in), 2 weeks and 12 weeks after treatment. Differences between VAR and PLA at different times were calculated with unpaired samples T test. Between-group differences in change from baseline to 2 and 12 weeks were evaluated with ANOVA analysis. RESULTS One patient (from group PLA) discontinued the protocol for lack of efficacy at 2 weeks. No differences between the groups in QOL questionnaire scores, uroflowmetry data or PVR were recorded at baseline. All enrolled men did not report any grade 2 adverse event. At 12 weeks, only 2 ( 6.9%) men in placebo groups and 3 (10%) in the vardenafil group reported persistent AEs. We reported significant differences between PLA and VAR for IIEF (2 weeks: 16,2 vs 18.7, p = 0,053; 12 weeks: 15.9 vs 19.4, p= 0,022), IPSS (2 weeks: 18.0 vs 14.9, p = 0,042; 12 weeks: 16.7 vs 12.8 , p= 0,014), IPSS-B (12 weeks: 3.8 vs 3.1, p= 0,045) and OAB-q (2 weeks: 18.2 vs 14.7, p = 0,000; 12 weeks: 17.7 vs 13.6, p= 0,006), while no significant differences resulted for uroflowmetry data and PVR. Furthermore, in VAR group after 12 weeks we observed a statistically significant increase in both Qmax and Qave (+2.4 mL/sec, p=0,025 and +1.0 mL/sec, p=0.042 respectively): this data was not present after 2 weeks of treatment. ANOVA analysis did not showed significant difference in change between PLA and VAR group for IPSS, IPSS-B and OAB-q, while it was found for IIEF (+0.33 vs +2.62, p=0,03), Qmax (+0.07 vs +2.44, p=0.034) and Qave (placebo: -0.15, vardenafil: +1.02, p=0.031). Moreover, 12 weeks treatment with vardenafil was associated with a significant change in mean irritative IPSS subscores (-1.68 vs -3.24, p=0.039), with no significance for obstructive IPSS subscores. CONCLUSION Vardenafil 10 mg combined with Tamsulosin 0.4 mg shows an excellent tolerability profile both at 2 and 12 weeks, in patients with persistent irritative urinary symptoms. As showed in the figure, this combination therapy allows to achieve significant improvement of erectile function, general and irritative urinary symptoms and bother compared to tamsulosin alone after 2 weeks of treatment. All These effects are further enhanced after 3 months of therapy. At 12 weeks a further improvement of both Qmax and Qave is obtained compared to tamsulosin alone. IPSS IIEF 25 24 23 22 * 20 * 21 19 Pla 18 Var 16 17 Pla 15 13 * 11 14 9 12 Var * 7 10 5 baseline 2w eeks 12 w eeks baseline OAB-q 2w eeks 12 w eeks IPSS-B 5 24 22 4,5 20 Pla 18 Var 16 4 Pla Var 3,5 14 * 12 10 baseline 2w eeks 3 * 12 w eeks * 2,5 baseline 2w eeks 12 w eeks