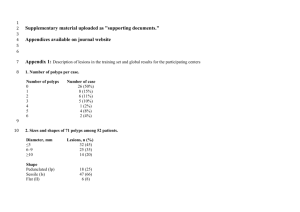
Is laparoscopic “oncologic” resection justified for patients with
advertisement

0099 Colon LESSONS FROM LAPAROSCOPICALLY-ASSISTED LARGE BOWEL RESECTIONS FOR COLONIC POLYPS Shpitz B, Neufield D, Tiomkin V, Ben Dahan G, Paran H, Benyamin B, Gutman M, Klein E. Departments of Surgery, Sapir Medical Center, Meir General Hospital, Kfar Sava, and the Tel Aviv University Sackler School of Medicine, Tel Aviv, Israel Background. One of the indications for laparoscopic segmental resection of the large bowel, are sessile colonic polyps not amenable for colonoscopic resection. Two major reasons for this approach are the resection of premalignant adenomas and the possibility that these lesions contain invasive carcinomas. There is a tendency to perform a limited segmental resection in patients with a presumably benign colonic polypoid lesions. The aim of our study was to evaluate the effect of an “oncologically-based” approach to such polyps in a cohort of patients who had undergone a laparoscopically-assisted colectomy for sessile polypoid lesions. Methods. A retrospective investigation of 25 patients who had undergone a laparoscopic colonic resection to deal with a large sessile adenomatous polyp which was not amenable to colonoscopic resection. All patients had undergone laparoscopically-assisted resections of the involved bowel segment with an extracorporeal functional stapled anastomosis for right colectomies and a double-stapled end-to end anastomosis for left colectomies. Results. All 25 patients were referred for resection with a preoperative diagnosis of adenomatoid polyps with or without foci of cancer. The average age of the patients was 71.8 years (range 51-93). In 13 (52%) patients these polyps were located in the proximal large bowel. There were 12 right colectomies, one - transverse colectomy and eight left colectomies or anterior resections. The extent of colon resections were 13.8 cm for right, 15.4 cm for left and 13 cm for transverse colectomies. Final diagnosis showed adenomas in 12 cases, invasive carcinoma in the adenomas in 9 cases and three invasive carcinomas with residual adenoma in three cases. One patient had two synchronous invasive cancers located in the distal transverse colon. The average number of lymphnodes that were retrieved was 17 for invasive cancers, and 7.6 for carcinoma in polyp. Postoperatively, the diagnosis switched from benign polyps to invasive cancers in three patients (12 %). Conclusion. Almost half of the patients (48%) in our study harbored either a carcinoma in benign adenomatous polyps (36%) or invasive cancer (12 %) indicating that a considerable percentage of these patients will harbor a malignant disease. These data indicate that an appropriate oncologic resection is justified for patients scheduled for laparoscopic resections due to large sessile adenomatous polyps.