Professional Letter - International Myeloma Foundation
advertisement

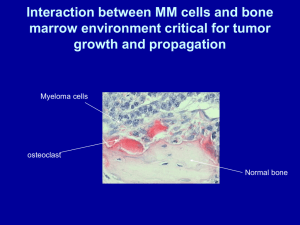
Understanding Multiple Myeloma Imagine experiencing back pain so severe that it keeps you in bed for weeks at a time. Imagine that someone has told you that you can no longer pick up your child or tightly embrace loved ones out of fear of breaking a bone. Imagine knowing that your symptoms could worsen to the point where you might become completely debilitated and that modern medicine, even with its breakthroughs, has no answers. Imagine that you have just been diagnosed with multiple myeloma. Multiple myeloma is a cancer of the bone marrow caused by the uncontrolled growth of plasma cells. Manufactured in the bone marrow, plasma cells are a critical part of the body’s immune system. In adults, the most active bone marrow is concentrated in the pelvis, spine, and skull, as well as in the long bones of the arms and legs. Normally, plasma cells make up less than 5 percent of the cells in the bone marrow, but individuals with myeloma have a significantly higher concentration of plasma cells in their bone marrow – greater than 10 percent and sometimes more than 90 percent. The danger associated with this high number of plasma cells stems from the fact that they are malignant and can invade and destroy the surrounding bone and displace the normal blood-producing cells in the marrow. The increased malignant plasma cells can actually dissolve bone, weakening areas of the skeleton and causing a severe osteoporosis-like appearance to the bones. The displacement of normal marrow causes anemia and reduced levels of white blood cells and platelets. Causes No single factor has been consistently associated with multiple myeloma. Overall it appears that certain occupations, as well as exposure to certain chemicals or radiation, can sometimes cause the disease in predisposed individuals. The diversity of possible exposures and genetic susceptibility factors make proof difficult. Recently, researchers have proposed infection, particularly viral infection, as a causal or trigger factor. Several studies have linked multiple myeloma to HIV, hepatitis, herpes virus infections (especially herpes virus 8), Epstein Barr Virus (EBV), as well as new “stealth adapted” viruses such as mutated cytomegalovirus (CMV). The significance of these viruses with regard to multiple myeloma remains to be fully explored. Signs and Symptoms Many multiple myeloma patients first visit their physicians with a complaint of pain along the lower back and ribs. Onset of sudden pain may be a sign of a fracture or collapse of a vertebral body caused by the excessive growth of malignant plasma cells and their destructive nature. In about twothirds of patients, anemia (lowered red blood cell count) is present at diagnosis. Approximately 30 percent of multiple myeloma patients may first begin to experience excessive tiredness, thirst and exhaustion caused by hypercalcemia – a condition in which high amounts of calcium are released as bone is dissolved, resulting in high levels of calcium in the bloodstream. Still others are likely to experience bruising, nose bleeds, hazy vision, headaches, gastrointestinal bleeding, sleepiness and a variety of neurological symptoms caused by reduced blood and oxygen supply to the nerve tissue. International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, California 91607 800-452-CURE (2873), 818-487-7455 818-487-7454 fax www.myeloma.org Patients with multiple myeloma often suffer complications such as pneumococcal pneumonia and deterioration of kidney function. The most serious complication is bone destruction, experienced by 80 percent of patients with multiple myeloma. Effects associated with the loss of bone density include brittle bones that can fracture easily and a severe loss of height. Without prompt and proactive management of the disease, the bone destruction becomes so severe that it leads to immobility. Diagnosis Multiple myeloma often is not diagnosed right away or is misdiagnosed by physicians. The average hematologist or oncologist may only see, at most, one to two new cases of multiple myeloma a year, and many will see none at all. For this reason, most cases are not diagnosed until six months to two years after the onset of the condition. In younger patients – those under 50 years old – diagnosis is often not even suspected because, until recently, the disease has been extremely rare within this age group. Diagnosis is made through a variety of means. Many patients are first diagnosed with multiple myeloma after routine blood or urine tests show high protein levels, which are caused by the overabundance of proteins secreted by the malignant plasma cells. Also common are unexplained anemia and recurrent infections. Physicians suspecting the possibility of multiple myeloma must confirm the diagnosis with two of the following three tests – all possible indications of multiple myeloma: o A bone marrow sample in which more than 10 percent (but usually greater than 20-30 percent) of the cells are plasma cells o A metastatic bone survey (series of X-rays covering the entire skeleton) that shows lytic lesions (holes in the bone) and/or diffuse loss of bone (osteoporosis) o A biopsy that reveals a plasma cell tumor inside or outside of the bone o Supporting diagnostic testing to identify the presence of the abnormal, monoclonal protein (M-protein) in the blood and/or urine Treatment Options Various treatment options are available to multiple myeloma patients, all of which are focused on reducing the degenerative effects of the disease and prolonging a high quality of life for the patient. Physicians will design an individualized treatment plan based on the patient’s disease characteristics. Because multiple myeloma currently has no cure, most patients seek treatment with other goals in mind. Various treatments may stabilize the disease, countering the potential life-threatening disruptions to the body chemistry and immune system. Other treatments mitigate the discomfort associated with multiple myeloma and can increase the patient’s ability to function normally. Some treatments can induce remission, lessening the severity of the symptoms and slowing or temporarily arresting the course of the disease. Remissions can last from months to decades. Permanent remission has rarely, if ever occurred. Many patients who achieve remission eventually die of progressive multiple myeloma and/or complications of treatment that typically include infection, kidney failure, bleeding problems, and intractable, complex cardiopulmonary conditions. Promising Research There is significant research currently being conducted to find a cure and better treatment options for multiple myeloma. Bank On A Cure®, the world’s first databank of myeloma-patient DNA, promises to help unlock the mystery of the disease. In addition, the International Myeloma Foundation received more than 30 grant applications this year for funding multiple myeloma research projects. With higher levels of research funding, it will be possible for physicians and scientists to study other very promising areas, including anti-angiogenesis agents, gene therapy, vaccines and anti-viral treatments. Hope for better treatment and outcomes is realistic. Multiple Myeloma Quick Statistics How many people suffer from multiple myeloma? GLOBAL - Daily: 1,000 new cases of multiple myeloma are diagnosed every day. UNITED STATES - Yearly: 15,000 estimated new cases in 2004: 7,000 women and 8,000 men. UNITED STATES - 75,000 – 100,000 multiple myeloma patients in the U.S. at any one time. Who gets multiple myeloma? Multiple myeloma is rare in children, teenagers and young adults. In adults, the likelihood of multiple myeloma increases with age. Peak incidences are in the 50s, 60s and 70s. Multiple myeloma is most common among people over 65 years old, with an incidence rate of 28.6 per 100,000 people vs. 1.8 per 100,000 people under 65. The prevalence within younger age groups is increasing, and at least 10 to 15 percent of patients are now under 45 years old. Multiple myeloma is more common in men. Multiple myeloma is more common in individuals of African descent. Incidence by race: o ~1/100,000 population/year: Asian o ~4/100,000 population/year: Caucasian o ~8-10/100,000 population/year: African descent What is the survival rate? Multiple myeloma is considered to be one of the fastest-growing types of cancer in the Western world. Individuals with multiple myeloma have a high mortality rate because there is no known cure for the disease. The median survival rate for patients is approximately three to five years following a diagnosis of symptomatic multiple myeloma. However, some patients live 10 to 20 years following their diagnosis, making outcomes unpredictable.