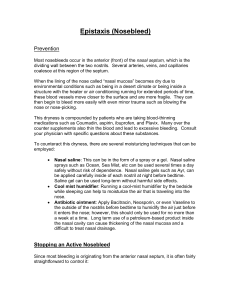
SURGERY 1: PLACEMENT INFORMATION
advertisement

SURGERY 1: PLACEMENT INFORMATION Welcome to Urology The Urology Department comprises of five Urological Consultants (Mr I Mitchell, Mrs R Webber, Mr K Janjua, Mr Blachandran (Locum) and Mr Chezzion (Locum)), one Urology Specialist Registrar (Alex Chapman), four Nurse Urology Specialists as well as staff in the ward, Urology Centre and theatre suites. There is one Urology ward (ward 54, Level 5) at Victoria Hospital. This in-patient ward for the department has 24 beds. Emergency referrals to Urology are assessed on the Admissions Unit 2 on the Ground Floor. The main theatre suite is located at Level 1. Urological operations are undertaken in theatre 10. Other activities at the Queen Margaret Hospital site include Urology Clinics that run on a Wednesday and Friday mornings in the main Outpatients Department on Level 1 adjacent to the Main Reception. A Wednesday lunch time Multidisciplinary Team (MDT) meeting is held in discussion room 1 located within the Education Centre next to ward 14 on level 2. The day case theatres for Urology flexible cystoscopy suite, investigations unit (scrotal and transrectal ultrasound and prostatic biopsies, urodynamics, general urology and specialist clinics in prostate assessment, haematuria, erectile dysfunction. Intravesical chemi/immunotherapy are all located within the Urology centre at the Victoria Hospital, (Ward 9, 2nd Floor, Phase 2) in Kirkcaldy. Due to limited time available every students will not be able to attend every area. Also clinical sessions may be changed or differ in the teaching content they provide. This will clearly affect what you see and learn but it is unavoidable when providing a patient led service in a busy specialty with a high turnover. The timetable will be given to you when you arrive on ward 54 on the first Monday afternoon. All of the core facts were given to you in Phase 2. This block will provide some clinical experience and a chance to revise and consolidate what you have learned in Phase 2. The aims of this part of the urology course are limited. They are: 1. To take a history and perform a physical examination on a patient assigned to you during the week. In selecting an appropriate patient it is advisable to ask the house officer or the Registrar. The case report should be written according to the instructions in the Phase 3, Year 4 Handbook. These would need to be handed back to Mr Byrne at Ninewells at the end of the week. 2. To attend a theatre session. This will involve observing open or endoscopic surgery. As well as learning from the operative case it is an opportunity to ask questions and discuss things with the medical staff. 3. To attend the Urology Centre for observing flexible cystoscopies. Here you will be asked to take a short urological history and perform a limited physical examination on a patient with haematuria, lower urinary tract symptoms (LUTS) or a history of bladder cancer. The student will then follow that patient into the endoscopy room and, in some cases, to the radiology department to observe a renal tract ultrasound examination. 4. To attend a urology clinic and observe consultations and perform examination in selected cases. Welcome to Ophthalmology Please report to the Cataract Unit at Queen Margaret Hospital on the 2nd Monday of your rotation at 10.00am. During your 7 days in the eye department you will send time in the outpatient department, theatre, local visual impairment society and in the education centre. Dr Blaikie is responsible for the overall running of the ophthalmology teaching blocks however there is usually a specific ‘named lead teacher’ for each block who you will see most of the time during your block. The aim of the teaching block is to try and make your comfortable with the common causes of red eye and visual loss, how to diagnose and manage these presentations. We also hope to be able to make you confident with the areas of ophthalmology that link in with general medicine including being able to recognise and grade diabetic retinopathy and make a decent effort at performing ophthalmoscopy as well as performing the other more specific ophthalmology examination techniques such as visual field examination and using the slit lamp. The Learning Objectives During your 7 day attachment in ophthalmology there are a small number of key learning objectives that you should try and ensure that you are familiar with at the end. These will be useful for your examinations as well as help you as a doctor when practicing after you graduate. 1. Take an appropriate history, perform a relevant examination, formulate a sensible differential diagnosis and initiate the management of the common causes of; a. red eye b. loss of vision 2. Become familiar with using a direct ophthalmoscope. 3. Be able to approach systematically the examination of the optic disc and develop a relevant vocabulary to describe the findings and then go on to be able to recognise the most common abnormalities. These include; swollen disc (papilloedema), cupping and optic atrophy. 4. Know the different clinical findings of diabetic retinopathy and be able to classify the different stages, in particular the difference between proliferative and non-proliferative diabetic retinopathy. 5. Know some basic facts about cataract and glaucoma which are two of the main conditions managed by ophthalmologists. The Didactic Lectures There will be 8 didactic lectures on the main ophthalmic subjects. These are mainly given in Dr Blaikie’s office in the cataract unit. The PowerPoint’s of these lectures are available on the University of Dundee Medical School website. Didactic Lecture List Introduction and overview Therapeutics Practical eye exam Practical ophthalmoscopy Loss of vision and neuro-ophthalmology Acute red eye and trauma Paediatric ophthalmology Glaucoma Diabetes There are many medical student orientated ophthalmology books on the market some of which are in the education centre library that you can use for reference and for your case reports. Assessment at the end of your ophthalmology attachment in Fife On the final afternoon of your ophthalmology teaching block (Tuesday pm) there will be an assessment session. This will include performing, discussing and marking an MCQ and a slide quiz with short answers. The marks from this will count for a small percentage of your final year result. Page 2 of 35 MCQ There are 20 questions with 5 stems. No negative marking. It takes about 15 to 20 minutes to complete then you will swap papers and mark each others as you discuss the questions and answers. It takes about 40 minutes to discuss the questions. Slide Quiz A few questions on 6 or 7 clinical pictures projected from a power point presentation. This also takes about 15 to 20 minutes. You will then swap papers, discuss the answers and mark each others. Case Reporting Marking Scheme During your 7 days you must identify a patient that you have seen and write up a brief case report. This should ideally be about 2 to 3 pages of A4 with a few diagrams or pictures if necessary. Try and find a patient on the first or second day so as you can write it up during the week. You are not supposed to do a cataract patient. You should hand it in on the last day. Key points in the case report include. • describing the presenting complain clearly • describing the full ophthalmic examination – Visual Acuities, slit lamp, fields, pupils, description of disc, macula etc • discussing the differential diagnosis • discussion, around the case which includes describing any surgical procedure and potential complications • should be properly research and referenced. Outcome Assessment Sheet Please hand in an outcome assessment sheet so your trainer can record your attendance and general attitude and knowledge for the medical school. Low Vision session with the Fife Society for the Blind Usually on the Tuesday afternoon of the first week a low vision session is arranged at the Fife Sensory Impairment Centre (FSIC). Within the FSIC building is the fife Society for the Blind (FSB). The session starts at 2pm and a map explaing the location of the FSIC is below. It is basically across the road from the Victoria Hospital in Kirkcaldy. Page 3 of 35 Page 4 of 35 Phase 3 2011/2012 Year 4 The Duke-Elder Undergraduate Prize in Ophthalmology If ophthalmology inspires you and you are thinking about it as a career then you could give the Royal College’s quiz (Duke Elder Undergraduate Prize) a try. This examination is intended for medical students who have completed their ophthalmology undergraduate teaching, but it is open to all medical undergraduates provided they have not graduated at the time of examination. Students may sit the examination on more than on occasion provided they have not yet graduated and have not previously won the prize. There will be a cash prize of £400 for the candidate gaining the highest mark. If there is more than one candidate gaining the highest mark this amount will be split respectively. There is no second prize. The examination consists of an extended matching question paper of 10 questions with 3 stems to each question. Candidates will have to pick their answer from a list of options. Marking is on the basis of +1 for a correct answer and -0.5 for an incorrect answer, and 0 marks for no answer or “don’t know”. The standard is high and candidates should anticipate a stiffer examination than encountered in the undergraduate class. Questions are mostly based on clinical ophthalmology but other areas covered include ocular physiology, anatomy and pathology as well as genetics of eye conditions and socioeconomic medicine relevant to ophthalmology e.g. blind registration or world blindness. Page 5 of 35 Phase 3 2011/2012 Year 4 Welcome to ENT ENT Study Guide Contents CURRICULUM OUTCOMES .................................................................................................... 6 ENT STAFF LIST ...................................................................................................................... 8 WELCOME ................................................................................................................................ 8 TIMETABLE: ............................................................................................................................. 9 BOOK LOAN ............................................................................................................................. 9 ASSESSMENT .......................................................................................................................... 9 INTRODUCTION ..................................................................................................................... 10 INFORMATION ACCESS ....................................................................................................... 10 OBJECTIVES OF AN ENT COURSE ..................................................................................... 10 MODIFIED ESSAY QUESTIONS ............................................................................................ 14 ENT FINAL ASSESSMENT .................................................................................................... 16 PATIENT PRESENTATIONS – NOTES FOR STUDENTS .................................................... 16 OTOLARYNGOLOGY AS A CAREER ................................................................................... 17 CAREERS IN RELATED SPECIALTIES ................................................................................ 19 CLINICAL METHODS IN OTOLARYNGOLOGY ................................................................... 21 HISTORY TAKING – EAR, NOSE AND THROAT ................................................................. 21 GENERAL ............................................................................................................................... 21 EXAMINATION – EAR, NOSE AND THROAT ....................................................................... 23 THE USE OF INSTRUMENTS ................................................................................................ 23 RECOMMENDED READING ................................................................................................. 26 CORE TEXTS:......................................................................................................................... 26 FURTHER READING: ............................................................................................................. 27 APPENDIX 1 - OSCE QUESTIONS........................................................................................ 27 PATIENT PRESENTATION YEAR 4 ...................................................................................... 34 Curriculum Outcomes Curriculum Outcomes What the doctor is able to do Good Medical Practice Keep your professional knowledge and skills up to date 1. Clinical Skills 2. Practical procedures Protect and promote health of patients Page 6 of 35 Phase 3 2011/2012 Curriculum Outcomes Year 4 Good Medical Practice and public 3. Patient investigation 4. Patient management 5. Health promotion and disease prevention 6. Communication Support patients in caring for themselves to improve and maintain their health Give patients the information they want or need in a way they can understand 7. Retrieve and handle information Treat patients politely and considerately 8. Understanding of basic, clinical and social sciences How the doctor approaches their practice 9. Appropriate attitudes, ethical understanding and understanding of legal responsibilities Make the care of your patient your first concern Treat patients as individuals and respect their dignity Respect patients’ rights to confidentiality 10. Appropriate decision making skills, clinical reasoning and judgement Listen to patients and respond to their concerns and preferences Respect patients’ right to reach decisions with you about their treatment and care Be honest and act with integrity 11. Role of the doctor within the health service Act without delay if you have good reason to believe that you or a colleague may be putting patients at risk Never discriminate unfairly against patients or colleagues The doctor as a professional Never abuse your patients’ trust in you or the public’s trust in the profession 12. Professional development Recognise and work within the limits of your competence Work with colleagues in the ways that best serve patients interests Page 7 of 35 Phase 3 2011/2012 Year 4 ENT Staff List Fife Consultants Associate Specialist Charge Nurse Departmental Secretary Dr K Haddow Miss L Hadoura Mr R Kelleher Mr D Walker Mr R Mountain Mr S Hakim Mrs M Robertson Mrs M Weir Ext 28526 Ninewells University Secretary University Technician Lorraine Warden Irene Bennett Ext: 32726 Ext: 33227 Consultants Mr Stephen Jones (Phase III Teaching Co-ordinator) Mr Quentin Gardiner Dr Kerry Haddow Mr Musheer Hussain Mr Suresh Mahendran Mr Sam Majumdar Mr Rodney Mountain Mr Peter Ross Mr Paul S White Specialist Registrars Mr Martyn Barnes Mr David Ellul Dr Phillip Jenkinson Miss C Kennedy Mr Mohammed Miah Mr Shwan Mohamad Administrative Assistant Sharron Lawrence Welcome Appendix 1 - For Students in Fife Welcome to the ENT department here in Fife. It is a small department with only 4 fulltime consultants and 1 Associate Specialist. We are part of a managed clinical network with Dundee and to facilitate this Mr Mountain, from Ninewells and myself have reciprocal sessions. We are also involved in a clinical network with Lothian for the management of head & neck cancer patients. The department closes from Friday Page 8 of 35 Phase 3 2011/2012 Year 4 afternoon to Monday morning with weekend emergency patients being looked after at Ninewells. The department in Kirkcaldy is integrated with inpatient beds and clinic rooms in ward 8. Theatres are on the same level. We also run outpatient clinics at Queen Margaret Hospital. During this attachment you will have a number of ward sessions as well as being involved with clerking of patients and management of emergencies. You will be expected to work closely with the junior staff and these sessions should be approached as a valuable resource to understand all aspects of the inpatient workload including management of emergencies. They will also allow you to select a suitable case study. The daily ward round starts at 8.30 a.m. and the student timetabled to the ward should be present. Timetable: You should report to ward 8 at the Victoria Hospital at 9.30 a.m. at the start of the attachment. You will be given your timetable then. You will participate in outpatient clinics and theatre sessions, which are arranged to help you understand a selection of the common conditions and operative procedures undertaken in ENT. You should also arrange to observe an audiogram being carried out – this should be easily possible in one of your clinic sessions. If you are interested you can arrange to observe an allergy clinic with our nurse practitioner. If you are allocated to the ward please attend the ward round at 8.30am but otherwise just come in for your theatre session or clinic at 9am. This ward isn’t big enough for you all to come to the round!! When you are on the ward you should help the GP trainees out with clerkings and observe the emergencies. Book Loan You will be given a core text book and a copy of John Diamond’s book “Because Cowards get Cancer Too”. These are required to be handed back prior to finishing your attachment. Assessment An end of block assessment will be available online. Details of how and when you can access this will be available during the block. Your written case report also needs to be finished by the end of the block and must be submitted to myself, my colleagues or to l.warden@dundee.ac.uk on the last day. If you have any concerns about this course please either let me know personally or contact Elspeth Dowling, Admin Assistant (Quality). I hope you enjoy your attachment Dr Kerry Haddow Consultant ENT Surgeon Page 9 of 35 Phase 3 2011/2012 Year 4 Introduction The importance of Otolaryngology, especially in relation to general practice is not always appreciated. A good working knowledge of the subject pays great dividends. Probably 10 - 20% of all patients seen in general practice have an ENT complaint. This means that at least two patients at each consulting session expose knowledge, or lack of it, in Otolaryngology. More than in almost any other field of medicine, practice in examination is necessary and the student should take every opportunity to examine as many patients as possible during this period of training. The methods described in this booklet are essentially practical and represent what we consider to be the most appropriate ones for your future career. Information Access . The departmental web site is at http://www.dundee.ac.uk/otolaryngology. This has information about the members of the department, information about the postgraduate teaching within the department, links to ENT related web resources and information for students, including material also hosted on Blackboard. There is also a link to the departmental blog (http://medblogs.dundee.ac.uk/ent) where up to date information for students, including changes to teaching, can be found and updates subscribed to. Objectives of an ENT Course Types of objectives: • Skill objectives • Attitudinal objectives • Factual knowledge objectives Methods • Ward work • ward rounds • clerking of patients Outpatients • • Outpatient Clinics at Victoria Hospital • Audiological testing at ENT clinic. • Allergy Clinic (nurse-led). • Tutorial Groups (Based on Study Guides) Page 10 of 35 Phase 3 2011/2012 Year 4 • Free Study in any spare time (Study Guides) • Modified essay questions Textbook “Ear, Nose and Throat and Head and Neck Surgery: An Illustrated Colour Text” by Dhillon / EastEar Skill objectives • To be able to examine the ear and recognise parts of the normal and abnormal pinna, ear canal, tympanic membrane and ossicular chain. • Tuning fork tests. • Other simple hearing tests (e.g. voice, watch). • Interpretation of audiograms. • Examination for nystagmus. Attitudinal objectives • Social and economic effect of deafness. • Problems of deafness in childhood. Factual knowledge objectives Ear disease • • • • • • • • • • • • • To be able to recognise otitis externa / acute otitis media. To be cognisant with the principles of treatment of common ear disease. To be able to differentiate between conductive and sensorineural deafness. To know the basic pathology and to be able to diagnose otosclerosis, tympanosclerosis, cholesteatoma and glue ear. To appreciate the relationship of adenoids and the Eustachian tube to middle ear effusion, cholesteatoma and ear discharge. To appreciate the place of hearing aids, environmental aids and hearing therapy. To know the first aid management of trauma to the ear. To know a list of common ototoxic drugs. To know how to manage a foreign body in the ear. To know a differential diagnosis and first aid treatment of the acutely painful ear. To understand the surgical approaches and anatomy of myringoplasty, ossiculoplasty, mastoidectomy, stapedotomy. To appreciate the relation between noise and deafness. To know a differential diagnosis of the discharging ear. Vertigo • • • • To know the basic physiology of balance. To be able to describe clearly what patients mean by “dizzy” attacks. To be able to list the main causes and pathogenesis of vertigo. To be acquainted with the methods of investigation of vertigo. Page 11 of 35 Phase 3 2011/2012 Year 4 Facial Nerve • • • • To be able to list the causes of facial nerve paralysis. To know the anatomy of the facial nerve. To appreciate the topographical diagnosis of facial paralysis. To understand the treatment of facial paralysis. Speech and Hearing • To be able to list the causes of deafness in childhood. • To know the milestones of speech and hearing. • To be able to describe and recognise simple speech disorders and retarded speech developments. Nose Skill objectives • To be able to examine the nose and recognise the septum, inferior and middle turbinates. • To know the normal colour of the nasal mucosa. • To recognise allergy, polyps and hypertrophied turbinates. • To know the principles of nasal packing. • To recognise Little’s area. • To know how to cauterise the nose. • To know how to assess the shape of the nose and abnormalities thereof. Attitudinal objectives • To have a perspective of nasal problems. • To appreciate the place of surgery in the treatment of nasal conditions. • To appreciate the psychological effects of cosmetic nasal and facial abnormalities. Factual objectives Epistaxis • To know commonest causes in each age group. • To know appropriate first aid and more specialised treatments. Allergy • To be acquainted with skin testing, desensitisation, etc. • To know the place of antihistamines, sodium cromoglicate, leukotriene modifiers and steroids in the treatment of allergic rhinitis. • To understand the treatment of nasal polyps. Page 12 of 35 Phase 3 2011/2012 Year 4 Nasal obstruction • To know commonest causes of nasal obstruction. • To understand basic principles of septal surgery. Sinusitis • To understand the pathology of rhinosinusitis. • To be acquainted with main treatment methods by antibiotics and nasal steroids. • To appreciate the value of radiological imaging Trauma • To be able to diagnose a fractured nose. • To understand principles of other facial fractures. • To know how to manage a foreign body in the nose. Facial Aesthetics • To understand the rules of facial proportions • To be able to assess the face for congenital or acquired deformity and understand methods of treatment • To appreciate when surgical treatments may not be appropriate • The role of psychology and psychiatry in facial aesthetics Pharynx and Larynx Skill objectives • To be able to examine the oral cavity and recognise normal structure, e.g. orifices of salivary ducts, tonsils, uvula, etc. • To be able to examine the throat, recognise the base of the tongue, palatine tonsils, and the posterior pharyngeal wall. • To demonstrate objective understanding of the post nasal space and laryngeal (epiglottis, supraglottis, glottis and subglottis) and hypopharyngeal anatomy when seen on endoscopy / indirect laryngoscopy. • To be able to examine the neck in a comprehensive and systemic manner. Attitudinal objectives • To realise the social and economic effects of major head and neck surgery. • To be aware of psychological factors involved in voice and throat symptoms Factual objectives Neck • To be able to describe a mass. • To know the main causes of masses in the neck. Page 13 of 35 Phase 3 2011/2012 Year 4 • To appreciate the proper place of cytology and biopsy. Sore throats • To know differential diagnosis of sore throat in children and adults. • To know the indications for removal of tonsils and adenoids. Dysphagia • • • • To know the normal swallow mechanism To know differential diagnosis of dysphagia. To appreciate the difference between organic and functional dysphagia. To know the different specialities that may be involved in the management of dysphagic patients Hoarseness • To understand basic voice physiology. • To know the colour and form of normal vocal cords. • To appreciate the difference between stridor, stertor, hoarseness and aphonia. • To understand the importance of early diagnosis of laryngeal cancer. • To understand the pathology of chronic laryngitis and the effect of social habits and occupation. Head and Neck Malignancies • • • • To have an awareness of signs and symptoms of cancer at each site. To understand the place of fine needle aspiration cytology / biopsy. To realise the significance of neck lymph gland metastases. To understand the treatment options employed in Head and neck Cancer management. • To understand the advantages and disadvantages of surgical oncology and medical / radiation oncology treatment options. • To have an idea of factors that affect 5 year survival rates and figures for the common malignancies. Respiratory Obstruction • • • • To understand tracheostomy and intubation. To appreciate the place of steroids in treatment airway compromise. To know how the principles of cricothyroidotomy. To know tracheostomy care. Modified Essay Questions These case histories incorporating questions, are designed to provide a practical approach to common E.N.T. problems (Appendix 1). At the same time you can test your own understanding of the problem. The subjects covered by these MEQ’s are: • Epistaxis Page 14 of 35 Phase 3 2011/2012 Year 4 • Nasal Problems • Adult Deafness • Childhood Deafness These should be done in your own time for free study - we suggest that you utilise part of the afternoons allocated to ward clerkships. Page 15 of 35 Phase 3 2011/2012 Year 4 ENT Final Assessment Case Study A “Case Study” based on your ward work sessions must be ready to be submitted on your last day. The written case presentation and discussion of the condition should cover no more than 3-4 sides of A4. Please ensure that the written case includes your name and matriculation number as well as a statement certifying that this is your own original work and your signature. The format of the case study should also include the usual headings you have been taught to use in any patient history and a references section at the end outlining any sources of information used in the preparation of your discussion. It is helpful if specific reference is made to the curriculum outcomes covered in your work. Please see the template for patient presentations in Appendix 3 of your 4th Year Student Handbook for the front page of your work. This is also appended at the end of this Study Guide. Online Assement Assessment will be carried out using online questions as in many other blocks. You will be advised of how to access it towards the end of the block and will have access made available to you. Marks at the end of the attachment will be based upon the online questions, written case study, any feedback from members of the department with whom you have had contact and regularity of attendance.Patient Presentations – Notes for students Your structured cases will be marked against the twelve curriculum outcomes. The following guidance may help you in completing the work. Outcomes Clinical Skills Record the history and clinical examination, describing the main findings and their interpretation in the different diagnosis. Practical Procedures Give a brief description of any procedure you were involved in, saying why it was performed. Patient Investigation Describe the investigations performed, summarise the results and interpret the findings. Patient Management Describe the management, noting any possible alternatives. Page 16 of 35 Phase 3 2011/2012 Year 4 Health Promotion / Identify and comment on examples of this (e.g. smoking Disease Prevention etc.) Communication Skills Describe the issues that were discussed with the patient, this may include written information about procedures. Retrieving and Handling Information Present your reports neatly and logically; describe any information retrieval, if appropriate. Basic Social and Clinical Science Identify any area where these helped your understanding of the case; these could be mentioned in the ‘lessons learned’ section at the end of the structured cases. Appropriate Attitudes, Ethical and Legal Understanding Make a note of any of these issues as they arise; again they may be included in the ‘lessons learned’ section. Clinical Reasoning Where appropriate, you can comment on how your case and Judgement required balanced judgement of alternatives. Role of the Doctor in the Health Service Issues of team working and professional responsibility can be described where appropriate. Personal Development The ‘lessons learned’ section gives you an opportunity to show how the case has contributed to your personal development. Otolaryngology as a Career Otolaryngology – Head and Neck Surgery is primarily a surgical discipline, but with a considerable medical component. It is concerned primarily with diagnosis and treatment of diseases of the upper aerodigestive tract. At one end of the career spectrum are specialists who concentrate on the management of head and neck cancer. The head and neck surgeon has to be skilled not only in surgery in general, but in the specialist aspects of extirpative and reconstructive surgery of the head and neck. At the other extreme is the audiological physician who may undertake no surgery, but who is concerned with the medical management of hearing loss, tinnitus and vertigo. Other sub-specialities in otolaryngology include otologic surgery, rhinology including both functional and cosmetic nasal surgery and bronchooesophagology. Paediatric otolaryngology is practised by some specialists as a discipline in its own right. Children account for one third of general ENT Page 17 of 35 Phase 3 2011/2012 Year 4 practice. The range of careers available is therefore wide and a degree of sub-specialisation at the Consultant level is becoming more common. Training requirements in Otolaryngology have evolved over the last few years. Following FY1 and FY2 training, which should ideally have given some exposure to surgical disciplines, entry to further training is competitive. Successful applicants will enter Core Training for two years (CT1 and CT 2), involving training in several surgical disciplines including Otolaryngology. Applicants must then go through a further interview process for Specialty Training. The Intercollegiate MRCS and the Diploma of Otolaryngology - Head & Neck Surgery (DO-HNS) is generally a requirement for entry to the ST level of training. Regulations with regard to entry requirement to each level of training are evolving and different patterns of appointment are emerging in different regions of the United Kingdom. There is an Intercollegiate fellowship examination which is taken towards the end of higher training. On completion of specialty training a certificate of completion of training is awarded and this allows the surgeon to apply for consultant posts. Nowadays most ENT surgeons undertake a degree of sub-specialisation and it is increasingly common for young surgeons to undertake fellowship training either in the UK or abroad. Competition for posts at all levels is extremely stiff and the aspiring surgeon should take advice from post graduate tutors, programme directors and the regional post graduate dean. Currently most otolaryngologists in the United Kingdom work in departments in district general or teaching hospital and there is an increasing tendency towards a smaller number of larger departments. This allows a greater degree of sub-specialisation and is likely to be the pattern of the future. Opportunities for academic practice in otolaryngology are variable. Several new chairs in the discipline have been established in the United Kingdom in the last few years. An increasing number of female graduates is entering what was previously a male dominated speciality and indeed two of the chairs created in recent years are currently occupied by female professors. Opportunities for private practice in otolaryngology vary in different areas of the country. Most private work is undertaken in private hospitals and some NHS hospitals offer limited private facilities. Further information regarding a career in otolaryngology may be obtained on an informal basis from the registrars or consultants in this Department. More detailed information is available from the Head of Department, from the Postgraduate Dean and from the British Association of Otolaryngology - Head and Neck Surgeons (BAO-HNS) (http://www.entuk.org/career_advice/). Page 18 of 35 Phase 3 2011/2012 Year 4 Undergraduate Essay Prize There is an undergraduate essay prize each year sponsored by ENT UK. Details are available at http://www.entuk.org/medical_students/medicalstudent_prizes/.Ca reers in Related Specialties Audiovestibular Medicine Some of the following is the information supplied by the British Association of Audiovestibular Physicians (BAAP) on their web site (http://www.baap.org.uk/) Audiological Medicine is the medical specialty concerned with the diagnosis and management of hearing - including tinnitus and other dysacauses - and balance disorders in adults and children. A broad general medical training allows appropriate investigation and medical management of the plethora of conditions that present with audio-vestibular symptoms. These include peripheral otological general medical, and central nervous system conditions, of varying aetiologies such as infections, inflammatory, vascular, traumatic and metabolic disorders. A multidisciplinary approach is key to the strong rehabilitative / habilitative aspect to the management of chronic disorders of hearing and balance disorders. Training in the specialty includes aspects of Developmental Paediatrics, Geriatrics, Medical Genetics, Neurology, Ophthalmology, Otolaryngology and Psychiatry, as well as an MSc in Audiological Medicine. This breadth of training facilitates continuing research and development in the speciality. Primary Career Structure This follows the general training pattern of consultant physicians. Basic medical training; foundation posts; higher professional training leading to Membership of the Royal College of Physicians, Membership of the Royal College of Paediatrics and Child Health. Specialist training in audiovestibular medicine in specialist registrar posts lasts five years. During this time trainees are recommended to complete an MSc in Audiological Medicine which may be carried out over one year of full-time study or two years of part-time study. There are currently two training rotations in the UK offering specialist registrar training in audiovestibular medicine. One is in the Thames region, the other rotates between Manchester, Sheffield, Nottingham and Cardiff. Local Provision In Tayside there is only one audiovestibular physician, Dr. John Irwin, who is based in King’s Cross Hospital. He also holds clinics in Perth Royal Infirmary. He teaches Dundee University Medical Students during the Phase 2 week and you may have met him then. Any students interested in attending an audiovestibular medicine clinic may be able to do so by prior arrangement. Please ask Lorraine Warden to contact him to see if this is possible during the block. Clinical SSCs are also available in this speciality. Page 19 of 35 Phase 3 2011/2012 Page 20 of 35 Year 4 Phase 3 2011/2012 Year 4 Paediatricians in Audiology Some of the following is the information supplied by the British Association of Paediatricians in Audiology (BAPA) on their web site http://www.bapa.uk.com Some Paediatricians (often Community Paediatricians) have a special interest in Paediatric Audiology and are involved in the identification, investigation of and ongoing management of children with hearing loss. The British Association of Paediatricians in Audiology (BAPA) is their professional Association. BAPA is a special interest group of the Royal College of Paediatrics and Child Health (RCPCH) and has taken up the challenge to work closely with the RCPCH on workforce planning, specialist training and development of competencies and standards for the paediatric speciality of audiovestibular medicine. BAPA also works closely with Government bodies in Scotland, England and Wales through representation on advisory bodies, small working groups and committees on matters relating to the delivery of paediatric audiology services. Local Provision In Tayside there are 2 paediatricians, Dr Ann MacKinnon and Dr Martina Stones, who work in partnership with Newborn Hearing Screening Service, Audiologists and the Otologists. In Fife Dr Barbara Scott provides a similar roleThey aim to provide a service for the early detection and effective management of children with any degree of hearing impairment in order to minimise the adverse effect that hearing loss may have on a child’s linguistic, emotional, social and educational development. When a child is confirmed as having a significant hearing loss there is further multidisciplinary working with speech and language therapy, education services and social services depending upon the individual needs and wishes of the child and family. Any students who are interested in visiting the newborn hearing screening service or attending a paediatric audiology clinic may be able to do so by prior arrangement. Please discuss with Lorraine Warden who will help with the organising this.Clinical Methods in Otolaryngology History taking – Ear, Nose and Throat General As in other areas of clinical medicine the scheme for taking a history is as follows: • Presenting details • Presenting complaint(s) • History of present illness • System review – this is usually confined to the other appropriate parts of the Head and Neck systems and any other bodily parts which seem relevant. Page 21 of 35 Phase 3 • • • • 2011/2012 Year 4 Past history Family history Social history Drug history Ears Deafness: time of onset, speed of onset, degree, unilateral or bilateral, progressive or static, fluctuation, past history of acoustic trauma, paracusis (ability to hear speech better in noisy places), distortion, family history. In children enquiry must also include details of the pre-natal history, birth history, and post-nasal history with special regard to the timing of speech and language milestone. Discharge: type, degree, side, frequency, odour, precipitating factors, duration. Pain: time and speed of onset, site radiation, precipitating or alleviating factors. Pruritus Tinnitus: frequency, side, character, duration, onset Vertigo: character, duration of each attack, falling, frequency of attacks, syncope, length of free periods, spontaneous, positional, associated manifestations, association with deafness, tinnitus, and feeling of fullness in the ear. Past ear infections, treatment and operations Ototoxic drugs: gentamicin, streptomycin, neomycin, kanamycin, quinine, etc. Facial weakness Headaches: site, frequency, severity Nose Nasal obstruction: side, periodicity, precipitating and alleviating factors, drug history, associated manifestations, seasonal or otherwise. Anterior nasal discharge: Watery, purulent, blood stained, odour, amount, precipitating or alleviating factors. Posterior nasal discharge (post nasal drip): “catarrh”, periodicity, associated manifestations. Epistaxis: anterior, posterior, side, duration, amount lost, periodicity, associated manifestations. Sneezing: precipitating factors, allergic associations. Anosmia: time on onset, unilateral or bilateral Past history of nasal operation Past history of nasal trauma Allergic history: seasonal (hay fever) or non-seasonal, family history e.g. eczema, chest complaints, precipitating factors. Drug history: hypotensive agents, proprietary nose drops etc. Associated features such as headaches, facial pain, sore throats, mouth breathing, snoring, epiphora, diplopia, voice change. Page 22 of 35 Phase 3 2011/2012 Year 4 Pharynx Sore throats: frequency, periodicity, site, duration, character, fever, dysphagia, odynophagia, cervical adenitis, effect of antibiotics, time off school/work, quinsy, state of general health. In children ask also about associated symptoms of adenoid hypertrophy such as nasal speech, deafness, snoring, nasal discharge and obstruction, dental occlusion. Dysphagia: true obstruction to swallowing or a feeling of discomfort on swallowing, food sticking, solids or liquids, time of onset, speed of onset, regurgitation, weight loss, progressive or stationary, heartburn and indigestion, past history of thyroid trouble, neck/injury, associated arthritis, reflux, vomiting, association with emotional state. Odynophagia: Pain on swallowing. May radiate to the ear. Mouth ulcers: Onset, duration, periodicity, single site or multiple, pain, radiation of pain, limitation of activities, cervical adenitis, associated manifestations. Loss of taste. Speech problems: stammering, dysarthria, dysphasia, dyslalia, clutter, stammer, structural abnormality in teeth or tongue or palate, hyper-nasality, hypo-nasality. Larynx Hoarseness: aphonia or dysphonia, onset, duration, periodicity, pain, progression, smoking habits, vocal abuse, associated chest illnesses, associated arthritis, occupational history. Stridor: inspiratory or expiratory, onset, duration, site Cough: sputum (quantity, appearance), haemoptysis, breathlessness, chest pain, ankle swelling, wheezing. Neck Lump in the neck: site, time of onset, duration, pain, getting larger or smaller, how discovered, association with other head and neck symptoms, gastro-intestinal symptoms, smoking habits. Thyroid history History of trauma Examination – Ear, Nose and Throat The use of instruments Forehead illumination The head mirror or head lamp. Forehead illumination require practice – especially the head mirror – but has certain advantages over other methods It gives stereoscopic vision The lighting is reliable (if mains supply is used) Page 23 of 35 Phase 3 2011/2012 Year 4 Forehead illumination is ideal for examining the mouth but this can also be done with a torch The head mirror should be good quality with a firm junction between the mirror and the head-band otherwise it is difficult to use. It should be worn the correct way up, i.e. with the hook from the head-bank pointing down. Wear it on the centre of the forehead and pull it down over the right eye. You will now see through the hole in the centre of the mirror with the right eye and past the side of the mirror with the left: the source of light which can be any reading lamp with 100w bulb, should be placed on the left side of the patient just above the level of his shoulder. The head lamp is easier to adjust and use: the light should be focussed to produce an intense spot (about 1 inch in diameter) at a distance of 8-12 inches. The patient should sit forward in the chair while being examined with his head slightly extended. The electric auroscopes A battery operated auroscope is the easiest way for a beginner to examine the ear. Magnification is very easily obtained which facilitates viewing the ear drum: it is impossible, however, to effectively carry out treatment through an auroscope, e.g. removal of wax, foreign bodies etc. Using the largest size of speculum it is possible to examine parts of the nose with an electric auroscope. The Ear Additional equipment • • • • • Specula: use the largest speculum which will fit the ear canal Seigle’s speculum: for testing drum mobility Tuning forks: 512 Hz should be used Probes with cotton wool for mopping Microscope Systematic examination • Examine the external ear, see it is of normal shape and for, look for postaural and endaural scars. • Ear canal - pull the pinna up and back to straighten the canal. Insert the auroscope speculum (turning it if hairs obstruct the view). Speculum, if correct size, will normally sit in the meatus without support. Note any discharge, wetness of the skin, presence or absence of wax. • Tympanic membrane - to examine different parts of the tympanic membrane the patient’s head will require tilting and the pinna may require pulling back. Note the handle of the malleus, short process, pars tensa, pars flaccida, colour, mobility, and any abnormality, e.g. retraction, perforation, discharge (smell). It may also be possible to see the incudostapedial joint and chorda tympani through a normal ear drum. Any of the following structures may also be seen through a perforation (or thin transparent scar), incus, stapes, Page 24 of 35 Phase 3 2011/2012 Year 4 stapedius tendon, promontory, round window. Get into the habit of drawing any abnormality seen. Tuning fork tests • The Rinne test: place the base of the vibrating fork firmly against the mastoid bone. When the patient no longer hears the note, place the fork by the meatus. Patients with either normal hearing or sensorineural deafness will hear the note again, i.e. air conduction hearing is better than by bone conduction. This is called Rinne positive. Those with a conductive deafness will not hear the note again and the test should be repeated in reverse order to prove that bone conduction is better than air. This is a Rinne negative response. • The Weber test: place the base of the vibrating fork on the centre of the forehead. Normally it is heard equally on both sides. With a unilateral sensorineural deafness the sound is heard better in the good ear. However, with a unilateral conductive deafness the sound is heard better in the poorer ear. If vertigo is also complained of examine for nystagmus getting the patient to look at a finger deviated 30º from the straight-ahead position on each side, check for Rhombergism and cerebellar signs. The Nose and Nasopharynx Additional instruments • Nasal speculum • Hopkin’s rod telescopes (if available) • Tongue depressor • Anaesthetic spray It is useful to employ an anaesthetic spray (lidocaine with phenylephrine) for every nasal examination since the solution will anaesthetise and shrink the mucosa of the nose and allow a more complete examination. Systematic examination • External nose: examine the shape of the nose from in front, the side and below. Note that the average naso-frontal angle is around 150º. The ala should be the same width as one eye and the ala should not extend beyond the medial canthus on each side. • Palpate the cartilaginous part of the nose to assess support. • Nasal cavity: (anterior rhinoscopy) - hold nasal speculum in the left hand, insert it into the nose and tilt the head according to the part of the nose to be examined. See if the septum is straight and the mucosa is a pink-colour. Note the inferior turbinates; in some patients you may be able to see the middle turbinate and middle meatus. Compare the airway on the right and left side. Note prominent vessels on the anterior septum (Little’s area) since this is a frequent site of epistaxis. If you are not sure if something is a polyp, palpate it (gently!) with a probe. Polyps are insensitive and floppy. Page 25 of 35 Phase 3 2011/2012 Year 4 • Often the view of the middle turbinate, middle meatus and the remainder of the nasal cavity to the nasopharynx is impossible to view by anterior rhinoscopy and a rigid or flexible endoscope is required. A rigid endoscope is preferable in the nose as it views at 30º from straight and allows a better view of the lateral walls and roof of the nose. The Mouth and Oropharynx Additional Instruments • Two tongue depressors • Glove for palpation • Always remove dentures if present Systematic examination • Start by examining the lips for cheilitis, tumour, etc. then employing two tongue depressors retract the cheeks and examine the gingivo-labial sulci, the teeth and the gums. Tell the patient to bite (back teeth) and note the occlusion. Retract the buccal mucosa laterally on each side and examine the parotid duct. Tell the patient to open the mouth and protrude the tongue centrally and then to either side to examine for surface lesions and mobility: examine the tip, the dorsum and the lateral surface of the tongue. • Put the tip of the tongue behind the upper teeth to enable examination of the under surface of the tongue and the floor of the mouth and the submandibular duct openings. Retract the tongue medially and open up the lateral floor of the mouth and look in the retromolar region. Malignant tumours of the oral cavity often start in this area. • Next examine the oropharynx: place tongue depressor on dorsum of tongue extending back as far as junction of anterior two-thirds and posterior third (approximately) depress it vertically, don’t tilt down the back. The tongue should not be protruded when using a depressor. Examine the tonsils. Note redness of pillars of fauces. Look for inflammation of the projecting part of the tonsil. In some cases use one tongue depressor on the tongue and squeeze the tonsil with the other to see if pus or debris can be expressed from the crypts. Look then at the hard palate and the soft palate, by asking the patient to phonate “ah” you will see the mobility of the soft palate. Look finally at the posterior pharyngeal wall. No examination of the mouth is complete without palpation of the floor of the mouth and tongue.Recommended Reading Core texts: • Ear, nose and throat and head and neck surgery : an illustrated colour text (3rd edition), Dhillon RS, East CA, Churchill Livingstone. ISBN 0443073112. • Master Medicine: Surgery: a core text with self assessment (3 rd Edition), Michael Lavelle-Jones, John Dent, Churchill Livingstone. ISBN 044310333X. Page 26 of 35 Phase 3 2011/2012 Year 4 • ABC of Ear, Nose and Throat (5th Edition), Harold Ludman, Patrick Bradley, BMJ Publishing Group. ISBN 1405136561. • Diseases of the Ear, Nose and Throat (Lecture Notes Series) (10th Edition), Clarke R, Bull PD, Blackwell Publishing. ISBN 1405145080. • Hall & Colman’s Diseases of the Ear, Nose and Throat (15 th Edition), Burton M, Leighton S, Robson A, Russell J, Churchill Livingstone. ISBN 0443061904. Further Reading: • Oxford Handbook of ENT and Head and Neck Surgery, Corbridge R, Steventon N, Oxford University Press. ISBN 0198564929. • Clinical ENT (2nd Edition) O’Donoghue GM, Narula AA, Bates GJ, Singular. ISBN 156593993X. • Master Medicine – Surgery 2. Ed. Dent J, Churchill Livingstone. Section 2 – Ear, Nose and Throat. ISBN 044307089X. • Colour Guide: ENT (2nd Edition), Stafford ND, Youngs R, Churchill Livingstone. ISBN 0443061467. • Diagnostic Picture Tests in Ear, Nose and Throat, Tony Bull, Mosby. ISBN 0723408432. • Case Presentations in Otolaryngology, McKenzie K and Dempster J, Butterworth-Heinemann. ISBN 0750613564. C: Because Cowards get Cancer Too, Diamond J, Vermillion. ISBN 0091816653.Appendix 1 - OSCE Questions Question 1 Mrs HW, aged 29 has been troubled by increasing bilateral deafness for the past five years of so. She has two children and noted that she became more deaf during her pregnancies. She has no other ear symptoms and in particular has never had discharging ears. She is quite definite that she heard normally until her early twenties. She also mentioned that she seems to hear quite well when she is in noisy surroundings. What is this phenomenon known as? 2 marks What sort of deafness does it suggest? Page 27 of 35 Phase 3 2011/2012 Year 4 2 marks What other important point in the patient’s history would you ask about? 1 mark What would the Rinne and Weber tests show in the case of conductive hearing loss affecting both ears equally? 2 marks What is the likely diagnosis in the above case? 1 mark How is the deafness caused? What treatment options could be considered? 1 mark Page 28 of 35 Phase 3 2011/2012 Year 4 2 marks Total 11 marks Question 2 Mr TS a 57 year old farmer is referred to Outpatients with a complaint of left sided epistaxis. On examination, a blood vessel was seen in Little’s area and cauterised. He was then sent home with instructions not to blow his nose for 24 hours. Which blood vessels anastomose in Little’s area? 2 marks Which method of cautery is usually used in outpatients? 2 marks Six hours later he arrives at the ward with a severe left sided epistaxis. On examination the nose had a great deal of clot in it and the bleeding was coming mainly down the front of the nose. What immediate first aid steps would you take? 2 marks First aid measures fail to arrest the bleeding and so an anterior nasal pack was inserted. Give one example of a commonly used nasal pack or material. Page 29 of 35 Phase 3 2011/2012 Year 4 1 mark His BP was 145/100 mmHg, Pulse 90 bpm, Temperature 36.8 ºC; no other abnormal signs were found on physical examination. Haemoglobin was 10.8 g/dl, film normal, platelets >100 x109/l Is any medical treatment indicated? 1 mark After two days the posterior and anterior packs were removed. Twelve hours later he had profuse bleeding from the left side of the nose. The bleeding was seen to be coming from the back below the middle turbinate. Which blood vessel supplies this area? 1 mark What treatment should therefore be offered? 1 mark Total 10 marks Question 3 Mr RH, a 28-year-old joiner, is referred to Outpatients by his G.P. with a complaint of nasal obstruction and recurrent sinusitis for the past year. He gave a history of nasal trauma sustained at football a year previously; since then he had constant difficulty breathing through the right side of his nose. His G.P. had treated him with Otrivine nasal drops and Sudafed tablets. What are the pharmacological names of these medications? Page 30 of 35 Phase 3 2011/2012 Year 4 2 marks What side effects could you expect from these? 1 mark He complains of four attacks of right-sided sinusitis during the past year. What symptoms might he complain of during an acute attack? 2 marks If you had examined him during an acute attack what main physical finding would you have expected? 1 markWhat drugs would you expect his G.P. to have used during an acute attack? 2 marks Anterior rhinoscopy shows the septum deviated to the right side and a large boggy red mass on the left side. It could be nasal polyp or a hypertrophied inferior turbinate. How do you differentiate these two conditions? Page 31 of 35 Phase 3 2011/2012 Year 4 1 mark You find that he smokes 30 cigarettes a day. How does this affect the course of rhinitis? 1 mark Total 10 marksQuestion 4 Mrs SM, female aged 74 is sent up to Ear, Nose and Throat Outpatient Clinic by her General Practitioner with a complaint of increasing deafness over the past few years. She manages adequately in ordinary conversation with adults but has great difficulty in a crowded room and with her grandchildren. What other symptoms would you ask her about in the first instance? 1 mark She thinks her hearing is equal in both ears. She has a hissing noise in both ears which is particularly troublesome at night. She has no vertigo, there is no history of otalgia or discharge. Why is her tinnitus bad at night? 1 mark What clinical tests and examinations are likely to be most helpful in suggesting a diagnosis? Page 32 of 35 Phase 3 2011/2012 Year 4 1 mark Her Weber does not lateralise. She is Rinne positive in both ears. What sort of deafness does she have? 1 mark This is her audiogram. Why did she have particular difficulty with a whispered voice and also with her grandchildren’s voices? Page 33 of 35 Phase 3 2011/2012 Year 4 1 mark She worked in a jute mill for 40 years. Has this affected the audiogram? 1 mark She is particularly worried about her tinnitus as well as the hearing loss. What treatments can you suggest that may be helpful? 2 marks To which other department might you consider referring her for the management of her tinnitus? 1 mark Total 9 marksPatient Presentation Year 4 Student's Name: System: Core Clinical as seen by doctor: Problem: as seen by patient: Supervising Consultant: Hospital: Date you first saw the patient: Page 34 of 35 Phase 3 2011/2012 Learning points in relation to the curriculum goals: (see over for further information) I certify that this patient presentation is my own original work. Signature of Student: _________________________________________ Page 35 of 35 Year 4