EPISTAXIS
advertisement

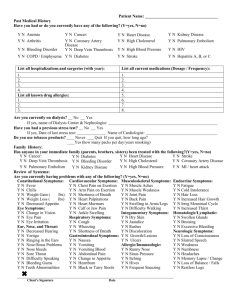
EPISTAXIS Never underestimate nosebleeds they can be fatal! The commonest ENT emergency by far. Causes: Unknown: in 80% of cases. The peak incidence occurs in children, young adults, and those 50 or over. There is a seasonal variation, nosebleeds are more common in cold weather. Trauma: Also common (nose picking) due to excellent vascularisation in Little’s area (close to the nasal opening Other: decreased haemostasis, haemophilia, excessive alcohol, Hypertension is not regarded as a cause although it can prolong bleeding. Ask about NSAIDS and anticoagulant use. Rare: hepatic coagulopathy, Osler-Weber-Rendu syndrome, leukaemia, malaria and typhoid. Management: ABC: First Aid: Further treatment: Anterior epistaxis: Posterior epsitaxis: Never forget ABC, always thinking of fluids. Resus the patient if necessary. unless the patient is shocked, have them sitting up with the head tilted downward to prevent blood trickling backwards. Firm pressure on the cartilaginous nose (not the bridge) for 1015 minutes Most nosebleeds will stop with pressure, but if not, try to visualise bleed. This is easier said that done. This is almost invariably septal. 1. remove clotts with suction, or by asking patient to blow their nose 2. insert a cotton wool pledget or a length of ribbon gauze soaked in a vasoconstrictor and/or local anaesthetic – into the nostril for 5 minutes. This should slow the bleeding and anaesthatise the area. 3. Obvious anterior bleeding can be cauterized with silver nitrate sticks. Warn that it stings. 4. Bleeding that persists can be treated with anterior packing with Vaseline and BIPP impregnated ribbon gauze or nasal tampons. Tends to be major or more severe than anterior. Watch out for shock, especially in the elderly. The gold standard treatment is visualisation with endoscopy and then cauterization. If bleeding site cannot be found, the nose may be packed with gauze. Bleeding arising more posteriorly usually requires posterior packing: Pass a 16-18G foley catheter through the nose into the pharynx, then inflate with 10ml of water, then pull until it get’s stuck. Then place an anterior pack, and secure it. Packing is generally left for 48h. There are well-recongised problems with infections and hypoxia. Therefore if packs remain in for >48h then consider close monitoring or prophylactic antibiotics Persistant posterior epistaxis: 1. Examination under GA. 2. Ligation