Historical review
advertisement

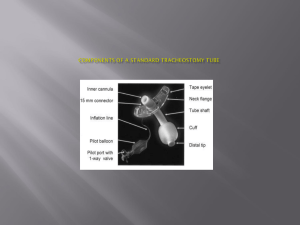
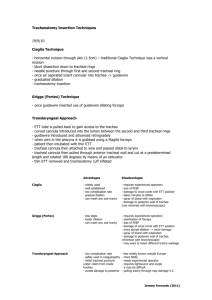
Laryngology Semina Tracheostomy & Tracheotomy 2004-10-27 R3 林正民 Historical review 2nd & 3rd centuries A.D.: Galen and Aretaeus. The first detailed reports of tracheotomy 1546: Antonio Muso Brasovolo. The 1st reported successful tracheotomy 1766: Caron. Remove a bean from a 7-year-old boy with tracheotomy Early 1900s: Bretonnear & Trousear. Tracheotomy for patients with diphtheria 1700s: Moreau:1st tracheotomy in recumbent position. (Prior to Moreau: Sitting position with neck hyperextension) 1909: Jackson C: Standard surgical principles of the tracheostomy—till now 1955: Shelden: 1st attempt percutaneous tracheostomy, fatality 1969: Toye & Weinstein: single tapered dilator 1985: Ciaglia et al: Percutaneous dilational tracheostomy (PDT) 1990: Grigg et al: PDT and guidewire dilating forceps (GWDF) Tracheotomy vs. Tracheostomy Anatomy of Trachea Tracheal diameter: 3mm (1-y-o) and increase with age. 2.0-2.5 cm (Adult). Flattened shape: Ant.—cartilageous rings, Post.—muscular membranous portion. 20 to 22 rings, with 2.1 rings per cm of trahea. Indications 1) Respiratory obstruction 2) Secretory retention 3) Resipratory insufficiency. Timing for intubation conversion to tracheotomy Post-intubational tracheal stenosis (Whited RE, 1984) < 5 days— No long-term laryngotracheal complications. 6 ~ 10 days— 5% chronic airway stenosis, vocal cords to cuff level. 11 ~ 24 days— 10 % laryngeal functional disturbance. 12 % chronic laryngotracheal stenosis. Medical Directors of Respiratory Care (Switzerland) (Plummer et al, 1989) a. Translaryngeal intubation preferred up to 10 days. b. Tracheostomy preferred when artificial airway is needed longer than 3 wks. Methods: Techniques, location, anesthesia 1. Cricothyroidotomy 1976, Brantigan and Grow 4% significant subglottic tracheal stensosis; 15% voice dysfunction 2. Minitracheostomy 14-gauge needle cricothyroidotomy with jet ventilation 3. Standard tracheotomy Emergency vs. Orderly tracheotomy Tracheal wall incision: a. Vertical b. Transverse c. Cruciate d. H type incision e. Horizontal H f. Björk flap g. Fenestation, window-type excision Tracheostomy in pediatric model: (Fry TL et al, 1985) Vertical incisionwas superior to horizontal H incision and Björk flap. Kremer B. (2002): recommend Björk flap to reduce danger of accidental decannulation and tracheostomal collapse while cannula exchange Tracheal incision Byrant LR (1978): No significant difference between window-type excision, transverse incision, and vertical incision with stoma stenosis. (Table ) Natvig KN (1981): Etiology of tracheal stenosismultifarious (Fig ) 4. Terminal tracheostomy: cervical or mediastinal 5. Percutaneous tracheotomy Currently, 25% of tracheostomy in ICU at USA. Needle (1st~ 3rd tracheal ring)Wire Dilator Tracheostomy tube (fig) Multiple serial dilation, ex Ciaglia Cook kit: (8 or 11 F38 F) Single-step dilation, ex Blue Rhino percutaneous tracheostomy kit Advantages of PDT over surgical tracheotomy— Smaller skin incision, less dissection and tissue trauma, fewer infection, decreasing risk and cost to OR, less time (11.7 vs 26.9min). Disadvantages — Higher perioperative complication (10% vs 3%) •Perioperative death (0.44% vs 0.03%) •Serious cardiorespiratory events (0.33% vs 0.06%) Contraindications to PDT Absolute—Emergent airway access, infants, infection at insertion site, high PEEP or oxygenation requirements Relative—Anatomic abnormalities (deviated trachea, enlarged superficial veins, etc.), enlarged thyroid or other neck mass, coagulopathy, previous neck surgery, obesity. Complications of Tracheostomy Intraoperative Early (< 7 days) Late (> 7days) Bleeding Tracheal laceration Tracheoesophageal fistula Tube malposition Recurrent laryngeal n injury Bledding Persistent abscess or cellulites, tracheitis Subcutaneous emphysema Pneumomediastinum Tracheoimmominate artery fistula Tracheoesophageal fistula Tracheal stenosis Tracheal malacia Pneumothorax Pneumomediastinum Cardiopulmonary arrest Tube malposition Tube obstruction Persistent Tracheocutaneuous fistula Reference 1. William W. Montgomery. Surgery of the larynx, trachea, esophagus, and neck. 2002. 2. Whited RE. A study of endotracheal tube injury to the subglottis. Laryngoscope. 1985 Oct;95(10):1216-9. 3. Plummer Al, Gracey DR. Consensus conference on artificial airways in patients receiving mechanical ventilation. Chest. 1989 Jul;96(1):178-80. 4. Burkey B, Esclamado R, Morganroth M. The role of cricothyroidotomy in airway management. Clin Chest Med. 1991 Sep;12(3):561-71. 5. Fry TL, Jones RO, Fischer ND. Comparisons of tracheostomy incisions in a pediatric model. Ann Otol Rhinol Laryngol. 1985 Sep-Oct;94(5 Pt 1):450-3. 6. Kremer B, Botos-Kremer AI, Eckel HE., et al. Indications, complications, and surgical techniques for pediatric tracheostomies. J Pediatr Surg. 2002 Nov;37(11):1556-62. 7. Marc S, Rovner. Percutaneous dilatational tracheotomy. Clin Pulm Med 2001;8(2):78-87. 8. Dulguerov P et al: Percutaneous or surgical tracheostomy: a meta-analysis. Crit Care Med 1999; 27: 1617-1625
![Chester _Royals_FCOT[1]](http://s3.studylib.net/store/data/006762869_1-d0409422479a6dd3b4d6752fba5dcd6e-300x300.png)