Problematic Urinary Tract Infections
advertisement

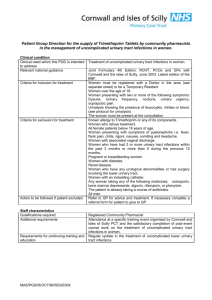
Guidelines for the treatment of problematic Urinary Tract Infections Introduction In an attempt to both minimize the spread of antibiotic resistance and to prevent the occurrence of Clostridium difficile, below are some recommendations for the management of problematic urinary tract infections. In the circumstances below it is important that patients are not started on any antibiotics, especially cephalexin, and left on them indefinitely. Management of Recurrent Urinary Tract Infections Recurrent UTIs need to be diagnosed by urine culture. Please advise on the request form that the patient has recurrent UTIs so that appropriate additional sensitivity testing can be carried out. Antimicrobial prophylaxis may be considered if a patient has two or more UTIs in a 6 month period or three or more in a 12 month period. If sensitive Trimethoprim 100 mg once daily or Nitrofurantoin 50 -100 mg once daily should be tried for 6 months then stopped. If recurrent urinary tract infections occur after stopping the prophylaxis AND the organisms grown are still sensitive to trimethoprim or nitrofurantoin; after treatment and eradication of organisms a further 6 -12 months of antibiotics may be tried. Notes on Recurrent Urinary Tract Infections NB see Spring 2012 edition of Path News for a more detailed discussion Antimicrobial prophylaxis for prevention of recurrent UTI should be considered only after discussion around behavioural modification has taken place including sexual and contraceptive practices, fluid consumption and cranberry products. In peri- and post-menopausal women and other women with low oestrogen levels atrophic vaginitis should be considered as a cause of urinary symptoms and managed as felt appropriate with oestrogens. Before any prophylaxis regimen is initiated, eradication of a previous uropathogen should be confirmed by a negative urine culture 1-2 weeks after treatment. If breakthrough UTIs occur while taking prophylaxis send urine for culture and if the isolate is not sensitive to the prophylactic agent stop the antibiotic prophylaxis. Continuous or postcoital antimicrobial prophylaxis may be considered to prevent recurrent uncomplicated cystitis in women in whom non-antimicrobial measures have been unsuccessful. The choice of antibiotics should be based upon the identification and susceptibility pattern of the uropathogens and the patient’s history of drug allergies. If uropathogens are not sensitive to trimethoprim or nitrofurantoin please discuss additional sensitivity testing results with the microbiology laboratory. For some patients with recurrent uncomplicated cystitis, self-diagnosis and self-treatment with a short course regimen of an antimicrobial agent may be considered as an alternative to continuous prophylaxis. There is evidence to suggest that cranberry is useful in reducing the rate of lower UTIs in women when used prophylactically but is not useful for treatment of UTIs. Management of Complicated Urinary Tract Infections A urine specimen for culture must be obtained before initiation of therapy and the selection of an antimicrobial agent should be re-evaluated once culture results are available. Trimethoprim is a reasonable first choice of antibiotic if the organism is susceptible. Other antimicrobials including Ciprofloxacin, Co-amoxiclav + pivmecillinam combination, may be needed if the organism is not sensitive to trimethoprim, or the patient fails to respond to trimethoprim, but these should only be prescribed after discussion with one of the medical microbiologists. Treatment for 7-14 days is generally recommended, but the duration should be closely related to the treatment of the underlying abnormality. Sometimes, a prolongation for up to 21 days, according to the clinical situation, is necessary. In males where a deep infection in the prostate or epididymo-orchitis is likely 2 – 6 weeks treatment is recommended. D:\681448807.doc Notes on Complicated Urinary Tract Infections Factors that suggest a potential complicated UTI The presence of an indwelling catheter, stent or splint (urethral, ureteral, renal) or the use of intermittent bladder catheterisation. Post-void residual urine of > 100 mL An obstructive uropathy of any aetiology e.g. bladder outlet obstruction (including neurogenic urinary bladder), stones and tumour Vesicoureteric reflux or other functional abnormalities Urinary tract modifications, such as an ileal loop or pouch Chemical or radiation injuries of the uroepithelium Peri- and post- operative UTI Renal insufficiency and transplantation, diabetes mellitus and immunodeficiency Complicated UTI can arise in a heterogeneous group of patients including: Patients in whom the complicating factors could be eliminated by therapy, e.g. stone extraction, removal of an indwelling catheter. Patients in whom the complicating factor could not be, or is not, removed satisfactorily during therapy e.g. permanent indwelling catheter, stone residues after treatment or neurogenic bladder. Intense use of any antimicrobial, especially when used on an empirical or prophylactic basis, in this group of patients with a high likelihood of recurrent infection, will lead to the emergence of resistant microorganisms in subsequent infections. Whenever possible, empirical therapy should be replaced by a therapy adjusted for the specific infective organisms identified in the urine culture. The successful treatment of a complicated UTI always combines effective antimicrobial therapy, optimal management of the underlying urological abnormalities or other diseases and sufficient life-supporting measures. Patients with pyelonephritis should be referred urgently to urology to investigate for obstruction. Asymptomatic bacteriuria Screening for and treatment of asymptomatic bacteriuria is recommended: For pregnant women Before an invasive genitourinary procedure for which there is a risk of mucosal bleeding Screening for, or treatment of, asymptomatic bacteriuria is not recommended for: Premenopausal, non-pregnant women Postmenopausal women Women with diabetes Healthy men Residents of long-term care facilities Patients with an indwelling urethral catheter Patients with nephrostomy tubes or ureteric stents Patients with spinal cord injury Patients with candiduria Screening for, or treatment of, asymptomatic bacteriuria in renal transplant patients beyond the first 6 months is not recommended. Pyuria in the absence of signs or symptoms in a person with bacteriuria should not be interpreted as symptomatic infection or as an indication for antimicrobial therapy. Guidelines on Urological Infections M. Grabe (chairman), T.E. Bjerklund-Johansen, H. Botto,B. Wullt,M. Çek,K.G. Naber,R.S. Pickard,P. Tenke,F. Wagenlehner © European Association of Urology2012 http://www.uroweb.org/guidelines/online-guidelines/ Scottish Intercollegiate Guidelines Network(SIGN). Management of suspected bacterial urinary tract infection in adults. Edinburgh: SIGN; 2012. (SIGN publication no. 88). [July 2012]. Available from URL: http://www.sign.ac.uk D:\681448807.doc