Rib Fracture Pain Management
advertisement

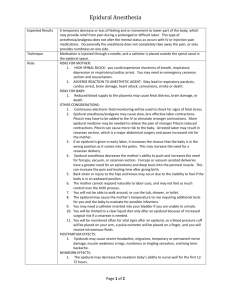
Genesys Regional Medical Center Trauma and Emergency Services Pain Management Guidelines in Blunt Thoracic Trauma Definition: Blunt thoracic trauma is defined in these guidelines as soft tissue trauma and injuries to the bony thorax such as rib fractures and flail chest. Preferred interventions: Pain control, chest physiotherapy, incentive spirometry and early mobilization are the preferred interventions for blunt thoracic trauma. Epidural analgesia is the optimal modality of pain relief for blunt chest wall injury and is the preferred technique after severe blunt thoracic trauma Indications: 1. 2. Patients with 4 or more rib fractures, who are > 65 years of age should receive epidural anesthesia Younger patients with 4 or more rib fractures or patients aged > 65 with lesser injuries should be considered for epidural anesthesia. Method: 1. 2. 3. 4. 5. 6. 7. Do not start Lovenox on patients with rib fractures. Lovenox may not be given for 24 hours before or after insertion of an epidural catheter. May use Heparin 5000 units subcutaneously q 8 hours Call Anesthesia main pager at 972 0227 Anesthesia will assess patient, obtain informed consent, choose appropriate medication and perform procedure. For break through pain a. call trauma surgery to assess reason for increasing pain b. call anesthesia to assess and treat. Anesthesia will round on patient daily. Adjuncts to pain control: 1. All patients with rib fractures not on the ventilator should perform Incentive spirometry every hour while awake. 2. Unless contraindicated by hemodynamic status, orthopedic or spinal column or cord injuries, all patients should be up in chair and preferably ambulated at least 3 times in 24 hours. 3. Oxygen protocol Monitoring: 1. Continuous pulse oximetry 2. Breath Sounds every 4 hours 3. Temperature every 4 hours 2005 Revised June 2007