Decompression Fasciotomies v1.2
advertisement

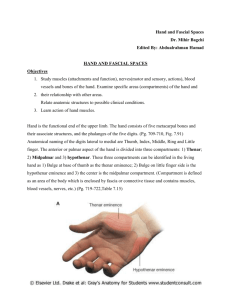
Peggers’ Super Summary of Decompression Fasciotomies Definition: A persistent rise in pressure within a confined fibro-osseous compartment that leads to partial or complete infarction and fibrosis of it’s contents LOWER LEG Compartments Compartment Anterior Indications: Clinical suspicion Delta P of 30mmHg Lateral Clinical assessment SYMPTOMS Severe pain unrelieved by analgesia Pain is persistent and progressive SIGNS Shiny tense skin Limb feels tense Nerve sensory from the nerve that transverses that compartment Passive stretch exacerbates pain Presence of pulse does not exclude compartment syndrome INVESTIGATIONS Pressure monitoring o Absolute value of 30mmhg for 8 hours or unknown period o Delta P of 30mmHg Blood tests o Ck suggests muscle necrosis (must also check U&Es) Anatomy: FINGER Mid-axial incision is dorsal to the n/v bundles HAND 10 compartments Extensor tendons Superficial radial nerve – 1st dorsal interossei region Deep motor branches of the ulnar and median nerves Palmar arch at Kaplan’s line FOREARM Forearm flexors Superficial – proximately PT and then FCR, Palmaris longus and FCU Intermediate – FDS Deep – FDP & FPL Deep and distal - PQ Forearm extensors by compartment Proximately – supinator and brachioradialis 1st – abductor pollicis longus and EPB 2nd – ECRL (2nd MC base) ECRB (3rd MC Base) 3rd – EPL 4th – Extensor Digitorum & Extensor indicis 5th – Extensor digiti minimi 6th - ECU Deep Posterior Superficial Posterior Muscles Tibialis anterior Extensor hallucis & digitorum longus Peroneus tertius Peroneus longus & brevis Tibialis posterior Flexor hallucis & digitorum longus Popliteus Gastrocnemius Soleus Plantaris Neurovascular structures Anterior tibial vessels Deep peroneal nerve Superficial peroneal nerve Tibial nerve Posterior tibial Artery Sural cutaneous nerve Principles of Operative Treatment: REMOVE RINGS OF BRACELETS General anaesthesia Can use tourniquet for initial exposure BUT must deflate to examine muscle Incisions must be full length Design incisions to avoid direct exposure of nerves and tendons Minimise cutaneous nerve damage and preserve cutaneous veins If EPIMYSIUM of muscles appear tight also incise this Upper Limb Fasciotomy: HAND OVERVIEW 10 compartments 4 dorsal interossei 3 palmar interossei Adductor compartment (adductor pollicis of thumb) Thenar Hypothenar HAND INCISIONS Dorsal incision Decompresses all interossei and the also the adductor compartments Incisions are made between the 2/3 metacarpals & 4/5 metacarpals Retract the skin to release the 4 compartments between each metacarpal, the 3 palmar interossei are also here and the adductor pollicis is deep to index finger metacarpal (deep to n/v bundles) Tenotomy scissors are used on the ulnar boarder of the index finger MC to access the adductor pollicis must feel the posterior fascia of the PALMAR interossei give way to be in the compartment Tenotomy scissors are also used in each of the other compartments to spit the fibres of the dorsal interossei to gain access into the palmar compartment Page 1 of 2 Peggers’ Super Summary of Decompression Fasciotomies Palmar incision Decompresses both ulnar and median nerves And also Thenar and Hypothenar muscles Make a lazy S incision in the carpal tunnel then extend distally as a zig-zag (Brunner) if required Incise the fascia over then Thenar muscles Release Guyon’s canal is much more superficial than you think, superficial to the carpal tunnel Continue into the Hypothenar muscles, preserving the deep motor branches of the ulnar nerve and the ulnar artery as it divides into superficial and deep palmar arches Make a longitudinal midline incision on the extensor aspect of the forearm Examine the muscles systematically LOWER LIMB 2 longitudinal incisions designed to release compression and preserve medial perforators required for subsequent flap closure The medial incision is 2 cm posterior to the subcutaneous medal boarder of the tibia The lateral incision is halfway between the tibia and fibula FINGER Finger decompression occurs at the non dominant side of each finger at the mid-axial Bending the finger and placing a dot at each crease apex and joining the dots up with the finger straight creates the mid-axial line This is dorsal to the n/v bundles Continue inside dorsal to the near side n/v bundle and then onto the volar side of the flexor tendons and then dorsally to the far side n/v bundle The non dominant side of the finger is the ulnar side for the middle 3 fingers and radial side for thumb and little finger FOREARM Flexor Incision The distal incision is a 5cm continuation of the carpal tunnel and distal wrist crease along the ulnar side of the forearm Continue in a straight line to the radial side of the antecubital fossa To extend into the upper arm use the antecubital flexors crease to extend the incision into the radial side of the antecubital fossa The extension into the upper arm continues proximately over the posteromedial aspects of the biceps brachii to decompress the biceps compartment, brachial artery and branches of the brachial plexus Extensor incision Medial expose the superficial posterior compartment exposing the gastrocnemius Retract gastrocnemius and expose the fascia of the deep compartment, expose the muscles and explore the n/v bundle Laterally expose the fascia of the anterior compartment and examine the contents Follow the under surface of the anterior compartment fascia until the vertical septum is found and incise this to gain access to the lateral compartment Examine the lateral compartment Wound Closure: Closure of the wound occurs in stages via a bootlace approach Split skin grafts are other option which provide coverage and contracture and thus can be excised in stages. 8/10th dermatome is used, the graft is left for 5-7 days splinted and the donor site for 14 days with mefix blue gauze mefix (under surface mefix allowed to peel and trimmed as it does) Mark donor site size inject LA infiltration with adrenaline into donor site. Decide on dermatome width and jelly both dermatome and skin Use assistant to hold skin taught Start dermatome before hitting skin and continue until machine has left skin Post-operative rehabilitation: Mobilise only once graft taken and stable circa 1-2 weeks PT mobilisation for 6-12 to prevent adhesions and stiffness Night splints for 4-6 weeks to prevent contractures o i.e. ankle at 900 o Wrist at 20-300 of extension, MCPs at 60-700 flexion and IPs at 1800. Outpatient follow up: Dressing clinic until wounds heeled Review at 6 weeks and 3 months Excision of skin graft if patient wishes at 9-12 months Tendon transfer for function consider plastics referral Page 2 of 2