Molecular Approach For Diagnosis Of
Rickettsia:
A Collaborative Initiative By Dept. Of
Medicine & Microbiology
Dr. Faria Ferdouse
Thesis part student of M.Phil
(Microbiology)
Mymensingh Medical College
Rickettsial diseases are a group of infections
caused by the obligate intracellular bacteria
Rickettsia.
It is a Gram-negative, non flagellated, nonmotile, non-spore forming, highly
pleomorphic bacteria.
They are small, cocco-bacilli that can
present as cocci or bacilli. They comprise a
group of microorganisms that
phylogenetically occupy a position between
bacteria and viruses
The name Rickettsiaceae honors Haword
Taylor
Ricketts
for
his
brilliant
experiments. Ricketts, as well as another
famous rickettsiologist, Von Prowazek, died
of rickettsia during their study period
•From 1873 to 1920, 66% of 431 reported
cases resulted in death in USA by Rocky
mountain spotted fever.
During 1983-1998, Five to thirty-nine
deaths were reported annually to public
health authorities.
In 1918 R. felis was first detected in European cat fleas
(Ctenocephalides felis)
In 1990 rediscovered in the United States.
In 2003 In Asia, the first case of R. felis infection
reported.
Recently has been demonstrated in Brazil, France,
Germany, Texas, Mexico, Africa, Spain
In
1993, WHO reported that, these are major
causes of febrile illnesses throughout the AsiaPacific region, also present in several parts of the
Indian subcontinent.
From India in 2010 reported that 45.6% had
spotted fever group and 30.7% scrub typhus &
untreated cases can have fatality rates as high as
30-35%.
For
India, the reported numbers are an
underestimate due to lack of community based
data and non-availability of confirmatory
laboratory tests.
Rickettsial disease in India has been
documented from Jammu, Kashmir, Himachal
Pradesh, Uttaranchal, Rajasthan, Assam, West
Bengal, Maharashtra, Kerala and Tamil Nadu
Since
Bangladesh is very adjacent to the West
Bengal of India, it is very likely that the same
Rickettsia would be responsible for certain
illnesses such as PUO, however there is no
scientific studies in Bangladesh so far.
With this concept in the background, we
conducted this study aiming at the following
objectives:
General objective:
Diagnosis of Rickettsial infection by PCR and other conventional
diagnostic tool.
Specific objectives:
To screen the Rickettsial fever by Weil-Felix test.
To detect IgM antibody against Rickettsia specific antigen by
ELISA.
To diagnose Rickettsial fever by PCR using genus specific gene
gltA (citrate
synthetase) and 16s rDNA.
A
total of 155 clinicaliy suspected cases of
febrile illness was selected from inpatient and
outpatient department of medicine and
pediatrics of MMCH during the period from july
2012 to september 2013.
Blood was collected and from each of the
patient with standard
procedure in the
department of microbiology MMCH for Weil
felix test ,ELISA and PCR.
• All the samples are tested by Weil felix test.
In Weil felix test OXK,OX2 and OX19 strains of
proteus are used to detect rikettsial antibody
• ELISA was done only Weil felix test positive
cases.
• Rikettsial outer membrane lipopolysaccharide
antigen were used for detection of antibody.
•PCR was done for all the specimens (155)
TABLE I
Age & sex distribution
of the cases
Age
group
(n = 62)
Female
(n = 74)
Total
(n = 136)
Up to 15 years
09
17
26
15 to 30 years
36
35
71
30 to 45 years
23
22
45
>45 years
06
07
13
74 (48%)
81 (52%)
155 (100%)
Total
Male
Table II
Clinical features of the cases
Clinical
features
No. of presenting
cases
Percentage (%)
Fever
155
100
Headache
98
63
Body ache
65
41
Cough
12
7.7
Rash
03
02
Conjunctival Hge
01
0.6
Table III
Result of Weil-Felix test
Weil-Felix
Antigen
Weil-Felix
Test
Positive
Total tested
155 (100)
Weil-Felix positive
136 (88%)
OX-2 OX-K OX-19
47
All160,
1-320
09
(All 160,
1 – 320)
06
(All
160)
OX-2
+
OX-K
OX-2
+
OX-19
OX-19
+
OX-K
All
three
25
17
10
22
TABLE IV
Result of ELISA for IgM
Total tested
129 (100%)
ELISA for IgM Positive
31 (24%)
Table V
Result of PCR
Total tested
155 (100%)
PCR positive
61 (39%)
Table VI
Correlation of Weil-Felix and PCR
PCR
Positive
Negative
Weil-Felix test
Positive
Negative
59
02
77
16
Test
Sensitivity
Specificity
Weil-Felix
96.72
43.38
PCR
100
100
Considering PCR as gold standard
Table VII
Correlation of ELISA and PCR
PCR
Positive
Negative
ELISA
Positive
Negative
20
41
13
81
Test
Sensitivity
Specificity
ELISA
32.78
60.61
PCR
100
100
Considering PCR as gold standard
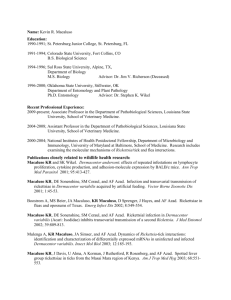
Rickettssia PCR
Date : 11/09/13
Primer : 17 K Da
Product size: 232
bp
232 bp
lane
01
02
03
04
05
06
07
08
09
10
11
12
13
14
15
16
17
Sl
no.
01
02
03
04
05
06
07
08
09
Ladde
r
10
11
12
13
14
15
16
Pos
Pos
Neg
Neg
Pos
Neg
Pos
Neg
Pos
Pos
Pos
Pos
Neg
Neg
Pos
For
confirmation of PCR product, Sequencing
was done at Sapporo Medical University using
Big Dye terminator.
1st email from Prof. Nobumichi Kobayashi
On Wednesday, October 23, 2013 3:48 PM, Nobumichi Kobayashi <nkobayas@sapmed.ac.jp>
wrote:
Dear Dr.Shyamal K. Paul,
How are you?
Salma arrived at Sapporo safely on Monday and started experiments on her study.
I received a souvenir from you, through Salma.
Thank you very much for it. We will try to taste it in our lunch or tea time.
Today Souvik tried to determine sequences of five PCR products from suspected
rickettsiosis brought by Salma. These five sequences were 99% identical to that
of Rickettsia felis.This Rickettsia distributes to cats, and infect to human via
cat flea.R. felis infection has been reported in some countries, but not in many
countries, thus seems to be still rare.
I guess probably all the specimens are clonal. This is very interesting finding.
Next week, Souvik will complete sequencing of all the pcr products and send you results.
Anyhow. please suggest Faria to search for literatures on R.felis as well as other common
Rickettsia, to facilitate preparation of thesis.
Sincerely,
N.Kobayashi
2nd email from Prof. Nobumichi Kobayashi
Dear Prof.Akram Hossain, Dr.Shyamal Paul,
Thank you very much for your message.
In my department, Souvik performed sequencing of 13 samples (2nd PCR products), out of 16 samples.
Three samples could not be sequenced and these products may be nonspecific amplicons. Attached
please find the original sequence data and alignment of 13 samples with Rickettsia felis strain,
GenBank KF241854, which shows 99% identity, with only one mismatch. (shown in color in the file)
Me and Souvik are now very busy, so further phylogenetic analysis will be done later.
Please send these data to the Mphil student, Faria.
I think that present study will be good enough for M Phil thesis as well as a good research paper in international
journal.
I have an idea for further study. Although detection of R. felis gene by nested PCR is highly interesting,
16S rRNA gene was not amplified, probably due to very less amount of Rickettsial cell in the blood
samples. Therefore, I would like to analyze more genes, to confirm and characterize R. felis in
Bangladesh. For this purpose, I would like to collect fleas from cats, i.e., wondring cats or those fed in
houses of patients. Of course because Rickettsia is very dangerous bacteria, we should pay high level of
attention for biohazards. Of course we never use them for culture. We should extract DNA from suspension of
fleas and do PCR only. This is just introduction of my idea.
Anyhow I hope to have good discussion and research activity when I visit MMC again.
If you have any plan of PCR for next time (in my next visit in January), please tell me in advance, because I will
prepare primers for it.
Sincerely,
N.Kobayashi
Sequence Alignment
Multiple alignment of 17 kDa antigen protein gene, partial cds, of Rickettsia felis strain, GenBank accession no. KF241854, with those of
Rickettsia strains detected in humans inBangladesh. R_felis
--TACTTGGTTCTCAATTCGGCAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 577
-TTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5813
-TTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5814
ATTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5925
ATTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5927
ATTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5932
---ACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5636
--TACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5740
--TACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5749
--TACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5767
-TTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5871
CATTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 6072
--TACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 5784
CATTACTTGGTTCTCAATTCGGTAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 60
****************** ************************************* R_felis
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 1177
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11813
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11814
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11925
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11927
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11932
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11636
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11740
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11749
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11767
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11871
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 12072
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 11784
CATTACTTGGAGCAGTTCTTGGTGGACAAATAGGTGCAGGTATGGATGAGCAGGATAGAA 120
************************************************************ R_felis
Sequence Alignment
Multiple alignment of 17 kDa antigen protein gene, partial cds, of Rickettsia felis strain, GenBank accession no. KF241854, with those of Rickettsia strains
detected in humans inBangladesh. R_felis
---TACTTGGTTCTCAATTCGGCAAGGGCAAAGGACAGCTTGTCGGAGTAGGTGTAGGTG 577
-************************************************************ R_felis
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 1777
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17813
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17814
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17925
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17927
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17932
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17636
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17740
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17749
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17767
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17871
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 18072
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 17784
GACTTGCTGAACTCACTTCACAAAGAGCTTTAGAAGCAACACCTAGCGGCACTAGCGTAG 180
************************************************************ R_felis
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAAA-- 2277
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--- 22713
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAAAAC 23014
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAAAA- 23025
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--- 22827
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATA---- 22732
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--- 22536
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAAA-- 22740
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAAC------------ 21749
AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA--AATGGCGTAATCCGGATAACGGTAATCATGGTTACGTAACACCTAATAA---
22667
22771
22972
22684
229
****************************************
Summary
And
Conclusion
A total of 155 clinically suspected febrile patients
were enrolled in the study. Out of them, 136 (88%),
31 (23%) and 61 (43%) were positive by Weil-Felix
test, ELISA and PCR respectively.
Out of the 61 PCR positive products, 16 were
sequenced in Sapporo Medical University, Japan
where 13 were found to be 99.9% consistent with
Rickettsia felis.
Considering PCR as gold standard, Weil-Felix
test is found highly sensitive (96.72%) but it
lacks good specificity (43.38%); whereas ELISA
has a moderate specificity (60.61%) but its
sensitivity is poor (32.78%).
PCR is considered as gold standard since currently
there is no provision for microscopy, culture &/or
IFA tests at MMC.
Further study
On the basis of these finding, we are now keen to
explore the relationship between the cat-flea and
the R. felis.
This study is now being conducted by
Dr. Rajib Ahmed,
Student of MPhil (Thesis part),
Dept. of Microbiology, MMC.
RECOMMENDATION
In our study, Rickettsia is found as an
important causative agent of febrile
illness especially the PUO.
So we recommend PCR as the
confirmatory diagnostic option of choice
for those cases of febrile illnesses which
is not confirmed to be caused by other
agents and when a preceding Weil-Felix
test is positive.
ACKNOWLEDGEMENT
Prof.
Nobumichi Kobayashi
Assoc. Prof. Shyamal Kumar Paul
Dr. Md. Chand Mahmud & Syeda Anjuman Nasrin
Dr.
Syed Ahmed Abdullah & Rajib Ahmed
All faculty members, fellow students, Lab.
technician & departmental staff
Physicians of Medicine Dept. who referred
the patients.
Overview of
Rickettsial fever
Classification
Rickettsiae
A
genus of small, rod-shaped, round to
pleomorphic microorganisms in the order
Rickettsiales.
They are true bacteria, gram-negative, and
cultivable only in living tissues.
Transmitted by lice fleas and ticks, they cause
disease in humans and domestic animals
Also found in the cytoplasm of tissue cells of lice,
fleas, ticks and mites, which may act as reservoirs
and vectors
Biological
features
Variable shape, coccobacilli
Gram negative
Microcapsule and slim layer
Culture : in yolk sacs of
embryonated eggs/ Tissue
culture
Rickettsia Transmission
Maintain in animal and arthropod reservoirs (ticks,
mites, lice, fleas by transovarian transmission).
Transmitted to humans by arthropod vectors
Humans are accidental hosts: acquired by arthropod
bite or contact of arthropod excreta with abraded skin
Pathogenesis
No toxins, no immunopathology
Rickettsia replicate in endothelial cells, cause
cell damage and blood leakage, vasculitis,
microthrombi, focal ischemia, hemorrhage, skin
rash.
Hypovolemia, hypoproteinemia, reduced
perfusion, organ failure.
Pathophysiology
Laboratory Diagnosis
Specimen:
Blood & skin biopsy.
Culture:
Tissue culture or chick embryo.
Direct detection in clinical specimen:
PCR
Immunofluorescence
Serological diagnosis:
Detection of rising titer of anti-rickettsial antibodies by ELISA.
Weil-Felix reaction: no longer used because it is non specific.
IFA reaction of a positive human serum on Rickettsia
rickettsii grown in chicken yolk sacs, 400X