Journal Club
Talmud PJ, Shah S, Whittall R, Futema M, Howard P, Cooper JA, Harrison SC, Li K,
Drenos F, Karpe F, Neil HA, Descamps OS, Langenberg C, Lench N, Kivimaki M,
Whittaker J, Hingorani AD, Kumari M, Humphries SE.
Use of low-density lipoprotein cholesterol gene score to distinguish patients with
polygenic and monogenic familial hypercholesterolaemia: a case-control study.
Lancet. 2013 Feb 21. doi:pii: S0140-6736(12)62127-8. 10.1016/S0140-6736(12)62127-8
Mozaffarian D, Lemaitre RN, King IB, Song X, Huang H, Sacks FM, Rimm EB, Wang M,
Siscovick DS.
Plasma Phospholipid Long-Chain ω-3 Fatty Acids and Total and Cause-Specific Mortality
in Older Adults: A Cohort Study.
Ann Intern Med. 2013 Apr 2;158(7):515-25.
2013年4月11日 8:30-8:55
8階 医局
埼玉医科大学 総合医療センター 内分泌・糖尿病内科
Department of Endocrinology and Diabetes,
Saitama Medical Center, Saitama Medical University
松田 昌文
Matsuda, Masafumi
Centre for Cardiovascular Genetics, Institute of Cardiovascular Science, University College London, London, UK
(Prof P J Talmud DSc, R Whittall MSc, M Futema BSc, P Howard BSc, J A Cooper MSc, S C Harrison MRCS, K
Li MSc, F Drenos PhD, Prof S E Humphries PhD); UCL Genetics Institute, Department of Genetics, Environment
and Evolution, University College London, London, UK (S Shah MSc, S E Humphries); NIHR Oxford Biomedical
Research Centre, Oxford University Hospitals NHS Trust, Oxford, UK (F Karpe PhD); NIHR School of Primary
Care Research, Department of Primary Care Health Sciences, University of Oxford, Oxford, UK (Prof H A W Neil
DSc); Centre de Recherche Medicale de Jolimont, Haine St-Paul, Belgium (O S Descamps PhD); MRC
Epidemiology Unit, Institute of Metabolic Science, Addenbrooke’s Hospital, Cambridge, UK (C Langenberg PhD);
Genetic Epidemiology Group, Department of Epidemiology and Public Health, University College London, London,
UK (C Langenberg, Prof A D Hingorani PhD); North East Thames Regional Genetics Service, Great Ormond
Street Hospital for Children, London, UK (N Lench PhD); Department of Epidemiology and Public Health,
University College London, London, UK (Prof M Kivimaki PhD, M Kumari PhD); Department of Epidemiology and
Population Health, London School of Hygiene and Tropical Medicine, London, UK (Prof J Whittaker PhD); and
Quantitative Science, GlaxoSmithKline, Stevenage, Hertfordshire, UK (J Whittaker)
Lancet. 2013 Feb 21. doi:pii: S0140-6736(12)62127-8. 10.1016/S0140-6736(12)62127-8
Background
Familial hypercholesterolaemia is a
common autosomal-dominant disorder
caused by mutations in three known genes.
DNA-based cascade testing is
recommended by UK guidelines to identify
affected relatives; however, about 60% of
patients are mutation-negative. We
assessed the hypothesis that familial
hypercholesterolaemia can also be caused
by an accumulation of common small-effect
LDL-C-raising alleles.
Methods
In November, 2011, we assembled a sample of patients
with familial hypercholesterolaemia from three UK-based
sources and compared them with a healthy control
sample from the UK Whitehall II (WHII) study. We also
studied patients from a Belgian lipid clinic (Hopital de
Jolimont, Haine St-Paul, Belgium) for validation analyses.
We genotyped participants for 12 common LDL-Craising alleles identified by the Global Lipid Genetics
Consortium and constructed a weighted LDL-C-raising
gene score. We compared the gene score distribution
among patients with familial hypercholesterolaemia with
no confirmed mutation, those with an identified mutation,
and controls from WHII.
cholesterol
9.16mM=354mg/dl 10.28mM=397mg/dl
5.87mM=227mg/dl 7.03mM=271mg/dl
4.22mM=163mg/dl 5.49mM=212mg/dl
1.42mM= 55mg/dl 1.37mM= 53mg/dl
TG
1.82mM=161mg/dl
1.33mM=118mg/dl
1.40mM=124mg/dl
6.4mM=247mg/dl
4.4mM=170mg/dl
4.4mM=170mg/dl
1.4mM=54mg/dl
T-chol <200mg/dl 0.0259 <5.18mmol/L
HDL-C >35mg/dl 0.0259 0.91 mmol/L
Triglyceride <250 mg/dl 0.0113 <2.8mmol/L
DNA was available from 451 patients with familial
hypercholesterolaemia without a known mutation from one
lipid clinic in Belgium, and 273 patients with familial
hypercholesterolaemia with a known mutation from the same
clinic. All patients had a cholesterol concentration above the
95th percentile for age and sex (appendix) and a family
history of early cardiovascular disease. The mean weighted
score of the mutation-negative Belgian patients (0・99 [SD 0・
19]) was significantly higher than the score of the WHII
participants (p=5・2 × 10−2⁰), with a smaller difference in
score between the mutation-positive patients (0・92 [0・20])
and the WHII group (p=0・04; appendix). The weighted score
in the mutation-negative group was also significantly higher
than in the mutation-positive group (p=4・0 × 10−⁶). Overall,
73 (16%) had a LDL-C gene score that fell within decile 10 of
the WHII LDL-C gene score distribution, and 211 (46%) fell
within deciles 7–10.
Polygenic familial hypercholesterolaemia: does it matter?
To add the complexity of SNP analysis for minor
genes and eliminate cascade LDL-C and clinical
testing of relatives of patients with polygenic
familial hypercholesterolaemia does not seem to
be warranted, and could even be diversionary.
*Evan A Stein, Frederick J Raal Metabolic and Atherosclerosis
Research Center, Cincinnati, OH 45227, USA (EAS); and
Department of Medicine, Faculty of Health Sciences, University
of the Witwatersrand, Johannesburg, South Africa (FJR)
February 22, 2013 http://dx.doi.org/10.1016/ S0140-6736(13)60187-7
Findings
We recruited 321 mutation-negative UK patients (451
Belgian), 319 mutation-positive UK patients (273 Belgian),
and 3020 controls from WHII. The mean weighted LDL-C
gene score of the WHII participants (0・90 [SD 0・23]) was
strongly associated with LDL-C concentration (p=1・4 ×
10−⁷⁷; R2=0・11). Mutation-negative UK patients had a
significantly higher mean weighted LDL-C score (1・0 [SD 0・
21]) than did WHII controls (p=4・5 × 10−1⁶), as did the
mutation-negative Belgian patients (0・99 [0・19]; p=5・2 ×
10−2⁰). The score was also higher in UK (0・95 [0・20]; p=1・6
× 10−⁵) and Belgian (0・92 [0・20]; p=0・04) mutation-positive
patients than in WHII controls. 167 (52%) of 321 mutationnegative UK patients had a score within the top three deciles
of the WHII weighted LDL-C gene score distribution, and
only 35 (11%) fell within the lowest three deciles.
Interpretation
In a substantial proportion of patients with familial
hypercholesterolaemia without a known mutation, their
raised LDL-C concentrations might have a polygenic
cause, which could compromise the efficiency of
cascade testing. In patients with a detected mutation, a
substantial polygenic contribution might add to the
variable penetrance of the disease.
Funding
British Heart Foundation, Pfizer, AstraZeneca, Schering-Plough, National
Institute for Health Research, Medical Research Council, Health and Safety
Executive, Department of Health, National Heart Lung and Blood Institute,
National Institute on Aging, Agency for Health Care Policy Research, John D
and Catherine T MacArthur Foundation Research Networks on Successful
Midlife Development and Socio-economic Status and Health, Unilever, and
Departments of Health and Trade and Industry.
Message
英国で、既知の関連遺伝子変異陰性の家族
性高コレステロール血症(FH)患者640人と
対照者3020人を対象に、低比重リポたんぱ
くコレステロール亢進アレル(LDL-Craising allele)の蓄積を発症原因の1つと
する仮説を症例対照研究で検討。LDL-C亢進
遺伝子変異の加重平均は、対照群に比べ患
者群で有意に高かった。
油脂の加工・精製でできるもの
EPA・DHA摂取量が多いほど
DPP-4阻害薬の効果が高い
魚摂取量
(%)
(%)
EPA摂取量
1.0
1.0
0.5
0.0
DHA摂取量
1.0
r=-0.616
p<0.01
HbA1c(NGSP)変化量
(%)
r=-0.618
p<0.01
r=-0.678
p<0.01
0.5
0.5
0.0
0.0
-0.5
-0.5
-1.0
-1.0
-1.5
-1.5
-0.5
-1.0
-1.5
-2.0
-2.5
0
40
80
120
-2.0
160 0
(g/日)
200
400
600
-2.0
800 0
(mg/日)
300
600
900
1200
(mg/日)
薬物治療を行っていない72例の糖尿病患者を対象に、DPP-4阻害薬を4ヵ月間投与し、食事内容の違いがHbA1cの低下
効果に及ぼす影響を検討した。
Iwasaki M et al., J Diabetes Invest 2012; 3: 464.
血中EPA・DHA濃度は
DPP-4阻害薬の効果予測マーカーとなり得る
(%)
血中EPA濃度
(%)
1.0
(%)
1.0
r=-0.675
p<0.01
HbA1c(NGSP)変化量
血中DHA濃度
1.0
r=-0.729
p<0.01
r=-0.323
p=0.165
0.5
0.5
0.5
0.0
0.0
0.0
-0.5
-0.5
-0.5
-1.0
-1.0
-1.0
-1.5
-1.5
-1.5
-2.0
0
50
血中アラキドン酸濃度
-2.0
100 150 200 250 0
(μg/mL)
-2.0
100 200 300 400 500 0
(μg/mL)
100
200
300
(μg/mL)
薬物治療を行っていない72例の糖尿病患者を対象に、DPP-4阻害薬を4ヵ月間投与し、HbA1cに及ぼす影響について
検討した。そのうち無作為に選択された患者における投与前の血中EPA・DHA濃度とDPP-4阻害薬による血糖低下作用
との関係についても検討した。
Iwasaki M et al., J Diabetes Invest 2012; 3: 464.
魚介類供給量と平均寿命の関係
(歳)
イタリア
84
豪州
スイス
82
日本
ニュージーランド
スウェーデン
フランス
ドイツ
カナダ
80
ギリシア
英国
78
平
均 76
寿
命
スペイン
アイルランド
オーストリア
オランダ
チェコ
アイスランド
ノルウェー
フィンランド
ポルトガル
韓国
デンマーク
米国
メキシコ
ポーランド
74
スロバキア
トルコ
72
70
0
10
20
30
40
50
60
70
80
90 (kg/人/年)
FAO「Food balance sheets」(日本以外の国)、農林水産省「食料需給表」、WHO「Statistical Information System
(WHOSIS)」に基づき水産庁で作成。
平成22年水産白書
In our study, the average daily
consumption of ω-3
PUFAs(polyunsaturated fatty acid)
from seal oil was ~8 g. We based
this estimate on a 30% ω-3 PUFA
content of seal oil.
Compared with less-than-daily consumption, both daily seal oil (odds ratio [OR] 0.2, 95%
confidence interval [CI] 0.1-0.8) and daily salmon consumption (OR 0.5, CI 0.2-1.1) were
associated with a lower prevalence of glucose intolerance, controlling for age, ethnicity, body
mass index, and sex. The effects were similar when limited to newly discovered cases: OR 0.3, CI
0.1-1.3 for seal oil and OR 0.4, CI 0.1-1.3 for salmon. Consumption of seal oil at least five times
per week was required to reduce risk.
Adler AI, Boyko EJ, Schraer CD, Murphy NJ.: Lower prevalence of impaired glucose tolerance and diabetes associated with
daily seal oil or salmon consumption among Alaska Natives. Diabetes Care. 1994 Dec;17(12):1498-501.
eicosapentaenoic acid (EPA).
1800mg/day
Kromhout D, Giltay EJ, Geleijnse JM; Alpha Omega Trial Group.: n-3 fatty acids and cardiovascular events after
myocardial infarction. N Engl J Med. 2010 Nov 18;363(21):2015-26.
Low-dose supplementation with EPA–DHA
or ALA did not significantly reduce the rate
of major cardiovascular events
Figure 2. Kaplan–Meier Curves for Primary and Secondary End Points. Kaplan–Meier curves are shown for the cumulative
incidence of major cardiovascular events (the primary end point) and fatal coronary heart disease (a secondary end point) among
4837 patients who had had a myocardial infarction and were assigned to receive a study margarine containing supplemental
eicosapentaenoic acid (EPA) combined with docosahexaenoic acid (DHA), a margarine containing alpha-linolenic acid (ALA), a
margarine containing both EPA–DHA and ALA, or a placebo margarine.
ORIGIN Trial Investigators, Bosch J, Gerstein HC, Dagenais GR, Díaz R, Dyal L, Jung H, Maggiono AP, Probstfield J, Ramachandran A, Riddle MC, Rydén LE, Yusuf S.: n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N Engl J Med. 2012 Jul 26;367(4):309-18.
n−3 fatty acids (popularly referred to as ω−3 fatty acids or omega-3 fatty acids)
are a family of unsaturated fatty acids that have in common a final carbon–
carbon double bond in the n−3 position; that is, the third bond from the methyl
end of the fatty acid.
eicosapentaenoic acid (EPA).
all-cis-4,7,10,13,16-docosapentaenoic acid (osbond acid)
all-cis-7,10,13,16,19-docosapentaenoic acid (clupanodonic acid) (DPA)
docosahexaenoic acid (DHA).
Conception and design: D. Mozaffarian, I.B. King, D.S. Siscovick.
Analysis and interpretation of the data: D. Mozaffarian, X. Song, H. Huang, F.M. Sacks,
M. Wang, D.S. Siscovick. Drafting of the article: D. Mozaffarian.
Critical revision of the article for important intellectual content: D. Mozaffarian, R.N.
Lemaitre, H. Huang, F.M. Sacks, E.B. Rimm, D.S. Siscovick. Final approval of the
article: D. Mozaffarian, R.N. Lemaitre, I.B. King, X. Song, H. Huang, F.M. Sacks, M.
Wang, D.S. Siscovick. Statistical expertise: D. Mozaffarian, H. Huang, M. Wang.
Obtaining of funding: D. Mozaffarian, R.N. Lemaitre, I.B. King, D.S. Siscovick.
Administrative, technical, or logistic support: X. Song. Collection and assembly of data:
D. Mozaffarian, X. Song, D.S. Siscovick.
Ann Intern Med. 2013;158:515-525.
Background:
Long-chain ω-3 polyunsaturated fatty acids (ω3- PUFAs),
including eicosapentaenoic acid (EPA) (20:5ω-3),
docosapentaenoic acid (DPA) (22:5ω-3), and
docosahexaenoic acid (DHA) (22:6ω-3), have been shown to
reduce cardiovascular risk, but effects on cause-specific and
total mortality and potential dose responses remain
controversial. Most observational studies have assessed
self-reported dietary intake and most randomized trials have
tested effects of adding supplements to dietary intake and
evaluated secondary prevention, thus limiting inference for
dietary ω3-PUFAs or primary prevention.
Objective: To investigate associations of plasma
phospholipid EPA, DPA, DHA, and total ω3-PUFA levels with
total and cause-specific mortality among healthy older adults
not receiving supplements.
Design: Prospective cohort study.
Setting: 4 U.S. communities.
Participants: 2692 U.S. adults aged 74 years
(±5 years) without prevalent coronary heart
disease (CHD), stroke, or heart failure at baseline.
Measurements: Phospholipid fatty acid levels
and cardiovascular risk factors were measured in
1992. Relationships with total and cause-specific
mortality and incident fatal or nonfatal CHD and
stroke through 2008 were assessed.
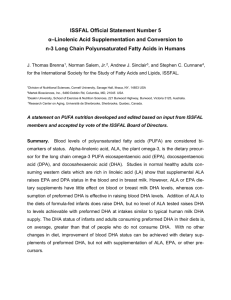
Figure 1. Multivariate-adjusted relationship of plasma phospholipid EPA, DPA, and
DHA levels with total mortality, evaluated using restricted cubic splines.
Figure 2. Relationship between dietary EPA plus DHA consumption and plasma
phospholipid EPA plus DHA concentrations, evaluated using restricted cubic
splines and adjusted for age, sex, race, and education.
Because the dietary questionnaire assessed only EPA plus DHA (and not DPA), for comparability we evaluated
circulating EPA plus DHA (rather than EPA plus DPA plus DHA) level. Median circulating levels of EPA plus DHA in
the highest quintile were approximately 5% of total fatty acids. The solid line and shaded area represent the
central estimate and 95% CI, respectively. There was strong evidence for both an overall trend (P < 0.001) and
nonlinearity of this relationship (P < 0.001). DHA = docosahexaenoic acid; DPA = docosapentaenoic acid; EPA =
eicosapentaenoic acid.
Table 4. Estimated Years of Remaining Life Gained After Age 65 y Among
Representative Older Adults, by Plasma Phospholipid Total 3-PUFA Level
PUFA polyunsaturated fatty acid.
* Values are the multivariate-adjusted estimated years of life gained after age 65 y in the highest
quintile of total 3-PUFAs compared with the lowest quintile and are based on semiparametric
survival models (see Table 3).
† This result is representative of a participant entering the study at age 65 y with average (mean)
values for each of the continuous covariates (body mass index [26.7 kg/m2], waist circumference
[96.8 cm], and leisure-time physical activity [1070 kcal/wk]) and falling into the most representative
category (mode) for each of the categorical covariates (sex [female], race [white], education [less
than high school], enrollment site [Forsyth County, North Carolina], fatty acid measurement batch
[2007–2010], smoking status [never], prevalent diabetes [no], prevalent atrial fibrillation [no],
Results: During 30,829 person-years, 1625 deaths
(including 570 cardiovascular deaths), 359 fatal and 371
nonfatal CHD events, and 130 fatal and 276 nonfatal
strokes occurred. After adjustment, higher plasma levels
of ω3-PUFA biomarkers were associated with lower total
mortality, with extreme-quintile hazard ratios of 0.83 for
EPA (95% CI, 0.71 to 0.98; P for trend = 0.005), 0.77 for
DPA (CI, 0.66 to 0.90; P for trend = 0.008), 0.80 for DHA
(CI, 0.67 to 0.94; P for trend = 0.006), and 0.73 for total
ω3-PUFAs (CI, 0.61 to 0.86; P for trend < 0.001). Lower
risk was largely attributable to fewer cardiovascular than
non cardiovascular deaths. Individuals in the highest
quintile of phospholipid ω3-PUFA level lived an average
of 2.22 more years (CI, 0.75 to 3.13 years) after age 65
years than did those in the lowest quintile.
Conclusion: Higher circulating individual and
total 3-PUFA levels are associated with lower
total mortality, especially CHD death, in older
adults. Primary Funding Source: National
Institutes of Health.
Limitation: Temporal changes in fatty acid levels
and misclassification of causes of death may
have resulted in underestimated associations,
and unmeasured or imperfectly measured
covariates may have caused residual
confounding.
Message
健常な高齢者2692人を対象に、長鎖オメガ3
多価不飽和脂肪酸(ω3-PUFA)と死亡の関
連をコホート研究で検証。血中ω3-PUFA高
値が全死亡率の低下と関連し、最低五分位
群に対する最高分位群のハザード比はエイ
コサペンタエン酸0.83、ドコサペンタエン
酸0.77、ドコサヘキサエン酸0.80、全ω3PUFA0.73だった。