Acid Base Disturbances – Dr Haber
advertisement

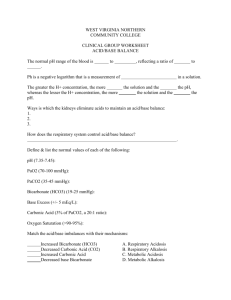
The Minimalist approach to acid/base disturbances ABG’s so easy….a GEICO rep can do it OBJECTIVES Acid/Base terminology and definitions Normal physiologic acid/base regulation Acid/base disturbances ABG interpretation Case studies Acid/Base terminology and definitions Acid/Base regulation / Control of( H+)concentration – Acid—proton (H+) donor increases (H+) – Base—proton (H+) acceptor decreases (H+) Ph is the logarithmic/exponential representation of (H+) concentration in eq/liter What is log???? 10 =10(1) log 10= 1 100=10(2) log 100=2 1000=10 (3) log1000=3 0.1= 10 (-1) log 0.1 = -1 0.01 = 10 (-2) log 0.01= -2 ph = - Log (H+) ph = 6 (H+) = 10 (-6) eq/liter eq/liter ph = 7 (H+) = 10 (-7) eq/liter 0.0000001eq/liter ph = (H+) = 10(-8) eq/liter 0.00000001 eq/liter 0.000001 H20 <<<<< (H+) + ( OH-) (H+) = 10(-7) eq/liter Pure Water has a ph 7(chemical neutral) Physiologic regulation of extracellular ph Normal physiologic ph = 7.4 Essential for normal enzymatic reactions Control Mechanisms/ Normal physiology Buffer systems (immediate) Respiratory (seconds) Renal (hours-days) Buffer solutions Solution of two or more compounds Prevent marked changes in ph when acid or base is added Bicarbonate Buffer H20 + CO2 <<< H2CO3 <<( H+)+ HCO3- Henderson/Haselbalch Equation ph = 6.1 + log HCO3-/ CO2 HCO3-/CO2= 20 Ph= 7.4 Ph is dependent on HCO3(direct) and CO2(inverse) HCO3 increases--- ph increases HCO3 decreases ---- ph decreases CO2 increases---- ph decreases CO2 decreases--- ph increase Physiologic Response to chronic acid load Bicarbonate Buffer system (immediate) – HCL + NaHCO3 >>>H2CO3 (CO2) +NaCL Pulmonary Control (seconds to minutes) – Ventilation of newly created CO2 in buffer system Renal control (hours to days) – Secretes H+ to reabsorb and regenerate HCO3 consumed by buffer Pathophysiology/ Acid/Base disturbances Acidosis---any process that lowers ph – Lowers HCO3- or raises PCO2 Alkalosis--- any process that raises ph – Raises HCO3- or lowers PCO2 Definitions Neutral – Ph 7.35-7.45 Acidemia – Ph < 7.35 Alkalemia – Ph > 7.45 More Definitons Isoelectric principle – + ions (cations) = -ions (anions) Anion Gap—(Na + K) – (CL + HCO3) nl =15 – Measures minor/unmeasured anions – Endogenous/exogenous anions Acid/Base disturbances Primary Secondary- a response to a primary disturbance – Opposite direction from primary – Compensation is partial and incomplete Acid/Base disturbaces Respiratory--- alteration in pCO2 Metabolic --- alteration in HCO3 Acute Respiratory AcidosisElevation in PCO2 CNS vs. pulmonary – CNS – coma, stroke – Pulmonary-asthma, COPD, pneumonia (very late) .08 ph drop for every 10mm increase in PCO2 – Typical abg’s 7.32/50/62 7.24/60/47 No metabolic compensation/ HCO3 unchanged Treatment- Fix the problem Chronic Respiratory Acidosis Chronic/slow PCO2 elevation – COPD/sleep apnea/obesity Compensatory metabolic alkalosis a major component – Kidneys increase H+ secretion –increase HCO3 .02 ph drop / 10 mm increase in PCO2 – Typical abg’s 7.38/50 /50 Treat underlying condition – Beware excess O2 7.36/60/55 Acute Respiratory Alkalosis/ decreased PCO2 CNS vs pulmonary – CNS stress, drugs, anxiety, sepsis, toxins – Pulmonary pneumonia/asthma/pulmonary embolism .08 ph increase 10 mm decrease in PCO2 – Typical abg’s 7.48/30/62 No metabolic compensation Treat underlying condition – Supplement O2 – Beware of paper bag Chronic Respiratory Alkalosis Extremely rare…some other time…. Acute Metabolic Acidosis Decreased HCO3 – Direct HCO3 loss via GI/kidneys – Decreased HCO3 from H+ buffering Metabolic Acidosis - defined by the associated anion Anion gap acidosis- increased minor anions – Endogenous/Exogenous Non anion gap acidosis-hyperchloremic – HCO3 loss from GI/kidneys – Increased reabsorption of CL- Acute metabolic acidosis Compensatory respiratory alkalosis Compensation is rapid but incomplete PCO2 drop= HCO3 drop – Typical abg 7.34/35/98 serum HCO3 =20 Treatment of Metabolic Acidosis Define and treat the underlying condition Watch for elevations in K+ Beware HCO3- Pitfalls of HCO3- treatment Paradoxical CNS and intracellular acidosis Over correction alkalosis Aggressive Na load Indications for HCO3- therapy HCO3 < 5 Ph <7.10 Cardiovascular instablity or irritability More likely to use on ventilated patients as CO2 is “blown off” Anion Gap Acidosis MUDPILES Methanol Uremia Diabetic (ketones) Paraldehyde Iron Lactate Ethylene glycol Salicylate Alternative Classification of anion gap acidosis Ketoacidosis Lactic acidosis Exogenous poisonings Uremia Ketoacidosis Diabetic alcoholic Diabetic ketoacidosis Insulin lack – Hyperglycemia – Fatty acid breakdown Ketone accumulation Treatment – Correct underlying disorder – fluids – insulin – maintenance of electrolytes especially K+ Alcoholic Ketoacidosis EtOH use followed by vomiting/starvation – Excessive ketone accumulation – Dehydration – Hypo or normoglycemia Treatment – Fluids – Maintenance of electrolytres – Glucose Lactic Acidosis Type A tissue hypoxia/underperfusion Type B abnormal lactate utilization Treatment Correct underlying cause – Antibiotics – Blood transfusion – Goal directed sepsis therapy – Fluids/pressors Exogenous toxins Alcohols – Methanol/ethylene glycol Salicylate Alcohol poisoning Ethanol not usually a major cause of acidosis MethanolEthylene Glycol – Formate/Oxylate accumulation – Increased osmolar gap – Renal failure/oxylate crystals Treatment for methanol/ethylene glycol – Ethanol drip – Dialysis Clues to diagnosis for ethylene glycol/methanol intox History – “sterno” or anti freeze ingestion Altered mental status Unexplained visual disturbances/coma Unexplained anion gap acidosis Renal failure Diagnostic Aides ABG/ HCO3 Serum osm ETOH level Osmolar gap Oxylate crystals Salicylate Toxicity Altered mental status Anion gap acidosis Primary respiratory alkalosis as well – Typical abg 7.35/20/110 serum HCO3 15 Treatment – Alkalinazation of the urine – K+ replacement – Dialysis Lab Evaluation of anion gap Metabolic Acidosis Ketones Salicylate Lactate Etoh/serum osm Osmolar gap = measured-calc serum osm Non Anion Gap-Hyperchloremic acidosis GI or renal HCO3- loss Compensatory CL- resorption Usually associated with hypo/hyperkalemia Metabolic Alkalosis Primary elevation in extracellular HCO3– H + losses from GI (vomiting) – Excessive renal H+ excretion/ elevated HCO3 resorpbtion – Exogenous ingestion Respiratory compensation – If HCO3 goes up by 10 pco2 goes up by 7 – Typical abg 7.47/47/100 HCO3 =34 Metabolic Alkalosis Physical effects – Tetany – Neuromuscular hyperactivity – Seizures – Decreased K+/ionized Ca 2+ Treatment – Correct underlying cause – Acetazolamide---causes renal HCO3 loss – Correct electrolytes ABG interpretation Step 1 obtain ABG/ HCO3- (electrolytes SMA7/Istat) Step 2 ph determination to determine – ph 7.35-7.45 = nuetral – ph < 7.35 = academia – ph > 7.45 + alkalemia Acidemia Flow chart to determine underlying process HCO3 low- primary process is metabolic acidosis pCO2 elevated- primary process is respiratory acidosis Metabolic Acidosis What is the anion gap???? Is the respiratory compensation appropriate – Appropriate PCO2/HCO3 =1 HCO3 =15/ PCO2 =30 – PCO2/HCO3 > 1 resp alkalosis HCO3=15 PCO2= 20 PCO2/HCO3 < 1 resp acidosis 15 PCO2 =43 HCO3= Respiratory Acidosis Is the acidosis acute/chronic? – Acute –ph down .08/10 mmPCO2 elevation – Chronic ph down .03/10mm PCO2 elevation – Acute on chronic 7.35/50/50 – Outside limits—second primary process Alkalemia flow chart HCO3 elevated- primary metabolic alkalosis pCO2 decreased- primary respiratory alkalosis Metabolic Alkalosis Is the respiratory response appropriate? – PCO2/HCO3 = .7 7.48/47/75 HCO3 =35 Respiratory Alkalosis Acute—is the ph response appropriate – Ph .08 up for every 10 mm decrease in PCO2 Nuetral ph Look for mixed primary disturbances – PCO2 – Anion gap – HCO3 Case studies Having FUN yet???/ Follow the flow charts!!!!! Case #1 57 y.o acutely SOB 7.32/60/55 HCO3=32 SMA 7 and anion gap otherwise normal Case #2 31 y.o homeless male unresponsive in park 7.24/29/107 Na 140 K 5.4 Cl 97 HCO3 14 glucose 110 Renal function normal Case #3 61 y.o with severe arthritis confused and agitated 7.34/18/110 Na 142 K 2.9 CL 99 HCO3 12 Glucose/renal function wnl Case #4 19 y.o. diabetic with vomiting 7.38/38/110 Na 140 K 2.8 CL 95 HCO3 24 Glucose 440 renal function wnl